Using the above described telemetry technique, we successfully recorded cardiovascular parameters in spinal cord injured animals. In animals with SCI alone, MAP was significantly reduced whereas HR increased compared to naïve animals, consistent with previous reports9. In animals with BS-NSC grafting, MAP and HR approached levels measured in naïve animals (Figure 2). During colorectal distension, a rat was regarded as dysreflexic if the noxious stimulation produced a rise in MAP and a decrease in HR3,8. Episodic hypertension and baroreflex-mediated bradycardia were inevitably triggered in all animals but the extent differed between groups. MAP increase in animals grafted with BS-NSCs was much lower (16.9 ± 3.1 mmHg, n = 3) than animals with injury alone (64.1 ± 1.6 mmHg, n = 3) (Figure 3). However, the decrease in HR during colorectal distension did not significantly differ between groups. As bradycardia is mediated by baroreflex mechanisms, this discrepancy may be due to reduced sensitivity of baroreceptors after SCI10. Spasm occurred during colorectal distension in most rats regardless of the treatment.
Upon histological analysis, immunolabeling indicated excellent graft survival in spinal cords implanted with BS-NSCs but a gap in the spinal cord of injured control animals without graft. Fetal NSCs completely filled the lesion site and only minor cavities were observed. Implants integrated into the host gray and white matter both rostrally and caudally. A large number of TH+ catecholaminergic and 5-HT+ serotonergic neurons were found within BS-NSC implants, and numerous axons topographically innervated caudal sympathetic preganglionic neurons in the intermediolateral cell column over long distances (Figure 4). In contrast, in injured animals without graft, TH+/5-HT+ fibers were not detected in thoracolumbar spinal cord below the lesion (not shown).
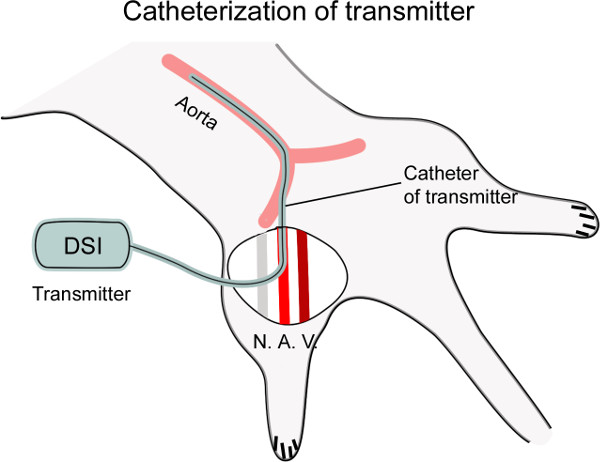
Figure 1: Diagram showing catheterization of the femoral artery. The femoral artery (A.) is dissected from the nerve (N.) and vein (V.), and then punctured with a curved needle. The catheter connected to the transmitter is inserted into the artery, placing the tip of catheter at the level of the thoracic aorta for cardiovascular recording (~4 cm).
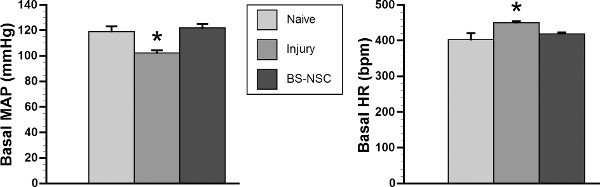
Figure 2: Basal MAP and HR recover in spinal cord injured rats grafted with BS-NSCs. In a representative cohort (n = 3/group), telemetry recording indicates significantly lower basal MAP and higher HR in rats with SCI and no treatment 10 weeks after injury (*p < 0.05). In contrast, both cardiovascular parameters recover to the level of naïve rats 8 weeks after BS-NSC grafting (10 weeks post-injury) (both p > 0.05; ANOVA followed by Fisher’s post hoc).
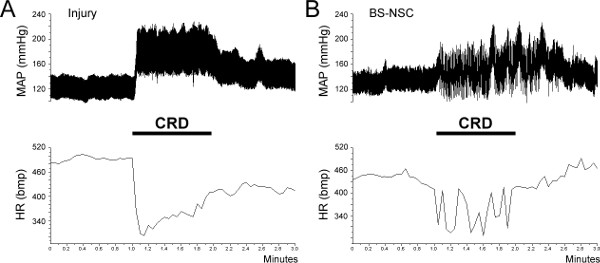
Figure 3: Colorectal distension (CRD)-induced autonomic dysreflexic. Autonomic dysreflexia is triggered during a 1 min CRD in both SCI and BS-NSC grafted animals, manifested as episodic hypertension accompanied by bradycardia. (A) In an injured control rat, MAP increases by approximately 60 mmHg during colon distension. (B) However, the increase of MAP is strongly reduced to 10 – 20 mmHg in a rat grafted with BS-NSCs.
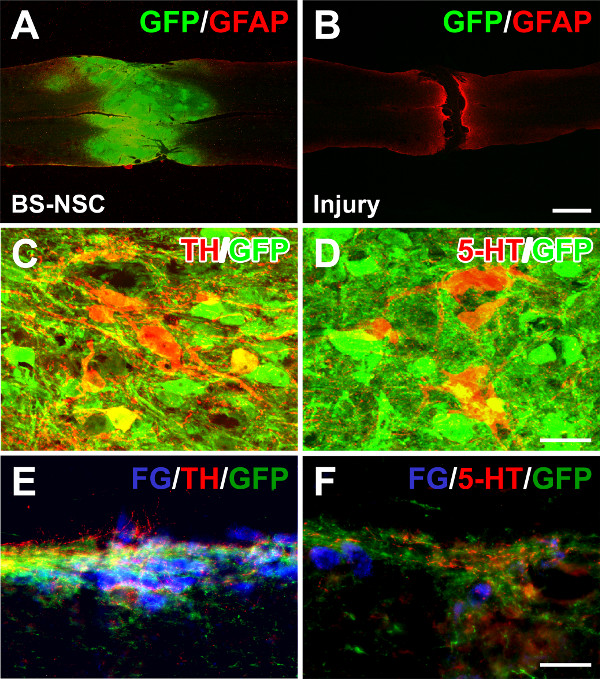
Figure 4: Grafted BS-NSCs integrate into the host adult spinal cord and differentiate into catecholaminergic and serotonergic neurons. (A) Eight weeks after BS-NSC grafting, GFP and GFAP double immunolabeling demonstrates filling of the lesion site with implanted GFP labeled cells in a longitudinal spinal cord section. (B) In contrast, a gap exists in a transected spinal cord without graft. (C, D) Immunolabeling for tyrosine hydroxylase (TH) and serotonin (5-HT) reveals many TH and 5-HT positive neurons within graft. (E, F) Graft-derived TH+ and 5-HT+ axons extend and innervate caudal sympathetic preganglionic neurons labeled with fluorogold in the intermediolateral cell column. Scale bars: 1 mm (B), 25 µm (D), and 50 µm (F).
