Computerized Neurocognitive Testing
An example of results for the computerized neurocognitive test can be seen in Figure 1. The computer program elicits composite scores on Verbal Memory, Visual Memory, Visual Motor Speed and Reaction Time which are often used to make return-to-play and return-to-learn concussion management protocols. The verbal and visual memory composites evaluate attentional processes, learning and memory. Visual motor speed measures visual processing, learning and memory and visual motor response speed (ImPACT Clinical Interpretation Manual). It also lists a Total Symptom Score at time of the test, an Impulse Control Score and a Cognitive Efficiency Index. The Impulse Control Score is related to the number of errors made in testing and may be useful in interpreting results. The Cognitive Efficiency Index attempts to measure the tradeoff between speed and accuracy. If the student-athlete experiences a concussion they are asked to come back in at 48 hr following concussion and when asymptomatic. Depending on the length of recovery the student-athlete may be asked to complete the assessment to examine recovery. It is assumed that following a concussion there will be significant decrements on performance on one or more of the composite scores and will recover to baseline when asymptomatic since this is often used as one indicator to return-to-play and return-to-academics.
Event Related Potentials
For the Flanker task participants are asked to respond to a middle arrow pointing to the left or right. This middle arrow may be going the same direction as the two flanking arrows (congruent) or opposite of the flanking arrows (incongruent). From the responses it is possible to determine response accuracy as well as response time to the arrows for congruent and incongruent. Additionally, from the brain activity being measured it is possible to derive an event-related potential (ERP). Figure 2 depicts the individual data for one subject on the Flanker Task. This data is derived from averaging across all the correct responses for the congruent and incongruent trials of the Flanker task. In examining the different ERP components one is typically interested in the amplitude and latency of the ERP component. Currently we are examining the P3, but we could also examine the N1, N2 and P2 components as well. The P3 typically occurs between 300–600 msec after stimulus presentation and is thought to represent context updating. The P3 can be quantified in amplitude, how high the peak is from baseline, and latency, how long the peak occurs from stimulus presentation. For the Auditory Oddball task it is also possible to determine response accuracy (number of correct responses) as well as response time to the high pitch tones (not the low pitch tones). Similar to the Flanker Task, ERP components and their amplitude and latency can be determined.
Figures 3 and 4 present preliminary data for the amplitude and latency of the P3 in the Flanker and Auditory Oddball tasks. One may expect that those who have suffered a concussion may have a larger amplitude and longer latency compared to their baseline or non concussed counterparts.
Somatosensory Perceptual Responses
Figure 5 illustrates a subject’s performance (difference limen) on an amplitude discrimination task with and without single site adaptation. Similar graphs could also be determined for simple single site reaction time task, dual site amplitude discrimination, a dual site amplitude task with a single site adapting stimulus and a temporal order judgment task. Individuals who suffer a concussion are expected to perform better on an amplitude discrimination task with a confounding single site adapting stimulus compared to non-concussed control subjects. An important point of emphasis is that a compromised neurological system (i.e. concussion) leads to better performance on some somatosensory testing tasks (including duration discrimination with an amplitude confound) which is a valuable contrast to the expected decrease in performance noted for other sensory and motor tests. Testing the somatosensory system can be performed quickly and may provide a sensitive measure to identify a concussion and track progress during the recovery phase to inform the return to play decision.
Balance
Figure 6 is a representative example of the results from the Balance protocol. The sway index and center of pressure data is used for further analysis. Table 1 shows the kinematic variables that are calculated from the center of pressure data and tells us more about balance control vs. just balance stability. Following a concussion balance and stability are often changed to either less stable (higher sway) or more stable (lower sway). Recovery would be when measures come back to baseline. Both changes can have implications on the ability to recover from or prepare for a loss of stability thus potentially putting a student-athlete at increased risk for injury.
Gait
Figure 7 illustrates the data output of a single subject. Data is compiled from the multiple trials and analyzed as one large walking pass. Table 2 includes the means and variability for gait measures across concussion history. One could expect that following a concussion the velocity and walking kinematics of a student-athlete will change. The implications of this in a dynamic task are far reaching. Gait parameters can help us understand how control of the system has changed and how it recovers.
Genetica
Table 3 is a sample output that is received after PCR analysis. Once this output is received genotypes can be determined for different participants and then equated with other variables such as concussion history, recovery from concussion and cognitive function. The current genotypes that are being determined include Apolipoprotein E (APOE), the polymorphic promoter region of APOE, Catechol-O-Methyltransferase (COMT) and Dopamine Receptor (DRD2).
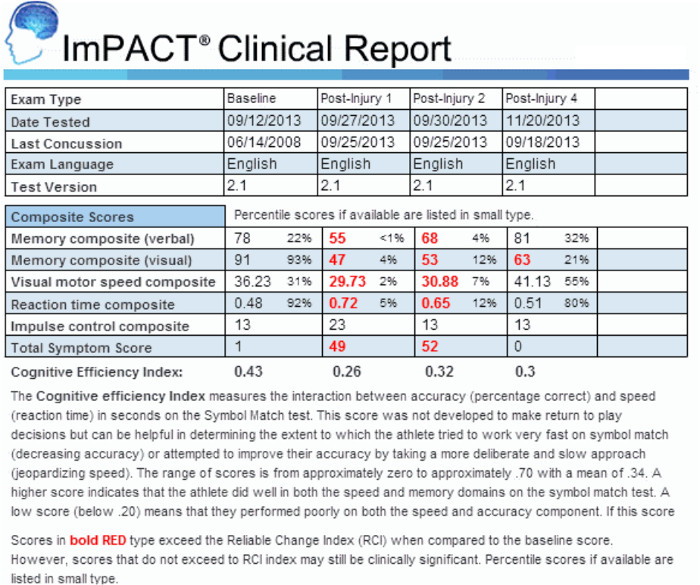
Figure 1: Example of computerized neuropsychological test report.
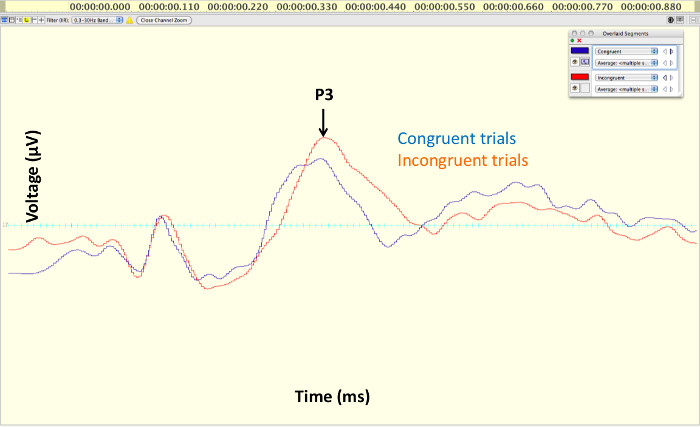
Figure 2: An example of a typical event related potential (ERP). The component of interest for the purpose of this investigation is the P3.
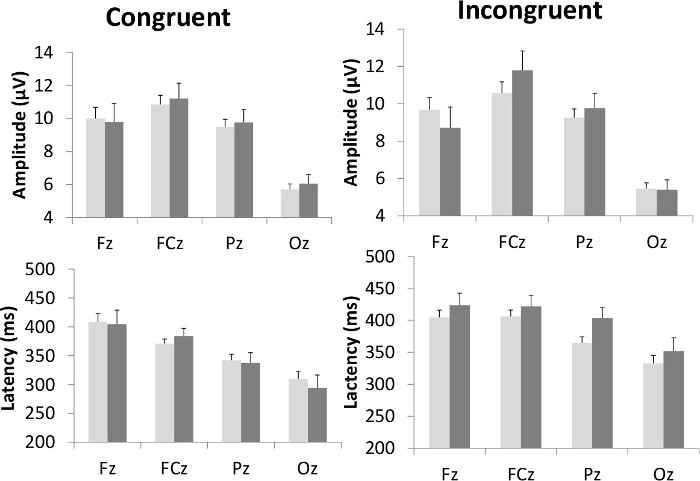
Figure 3: Preliminary results showing differences in amplitude and latency for P3 associated with the Flankers task. Results are presented from the midline electrodes associated with the frontal (Fz), frontocentral (FCz), parietal (Pz) and occipital (Oz) regions of the brain. Previously concussed subjects are indicated in dark grey while non concussed subjects are indicated in light gray.
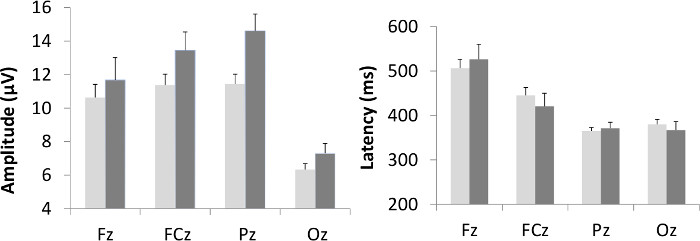
Figure 4: Preliminary results showing differences in amplitude and latency for P3 associated with the Auditory Oddball task. Results are presented from the midline electrodes associated with the frontal (Fz), frontocentral (FCz), parietal (Pz) and occipital (Oz) regions of the brain. Previously concussed subjects are indicated in dark gray while non concussed subjects are indicated in light gray.
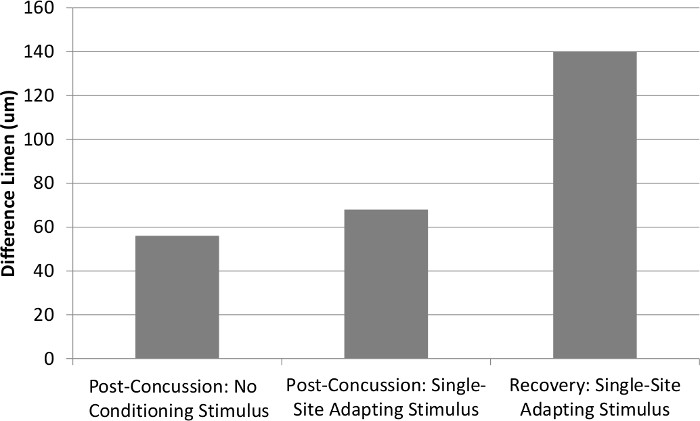
Figure 5: Comparison of difference limen for a single subject obtained with amplitude discrimination tasks with or without single site adaptation at post concussion and at recovery. The post concussion performance with a single site adapting stimulus is similar to the performance without a conditioning stimulus. However, in normal control subjects the presence of a single-site adapting stimulus leads to a decrease in performance (i.e., the difference limen increases); similar to the recovery performance.
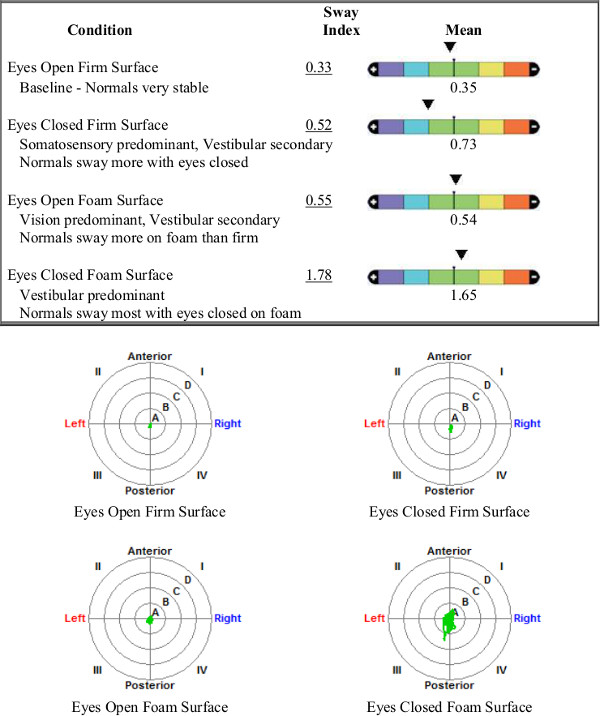
Figure 6: Example of balance test report. The top figure shows the sway scores as compared to normative data. The bottom shows the center of pressure data for each trial.
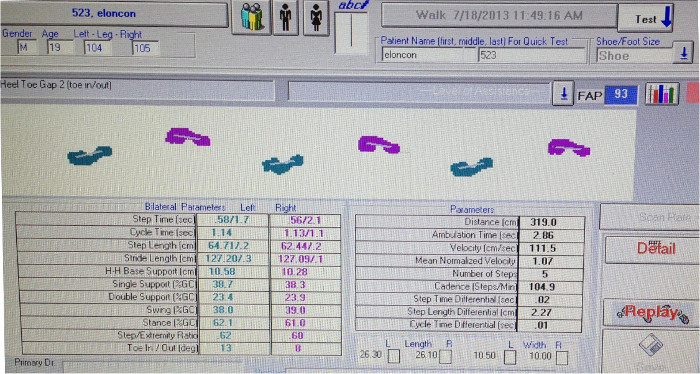
Figure 7: Example data produced by gait analysis system. The top is the foot pressure on the mat and the bottom has all the kinematic measures.
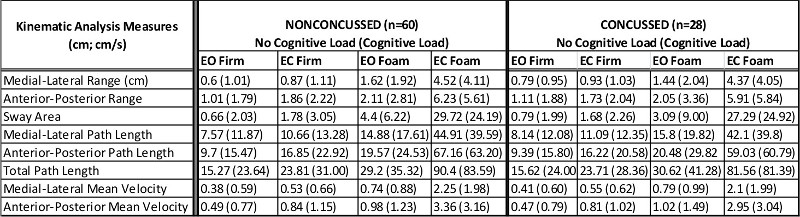
Table 1: Center of Pressure Kinematic Measures across conditions for a group of student athletes with and without a previous history of concussion.
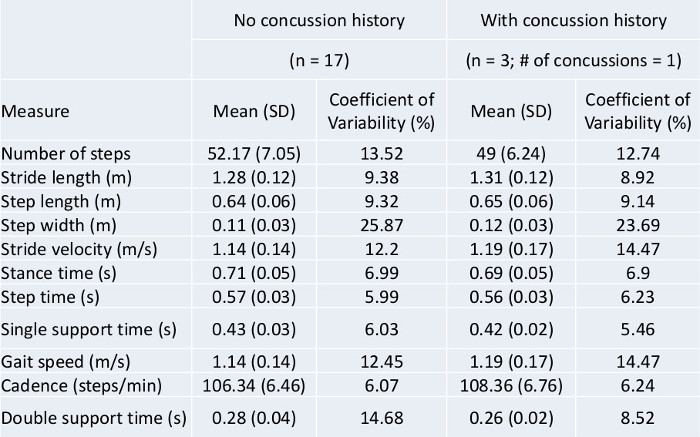
Table 2. Spatiotemporal parameters from gait evaluations of high school football players collected as part of the Elon BrainCARE protocol using gait analysis instrument
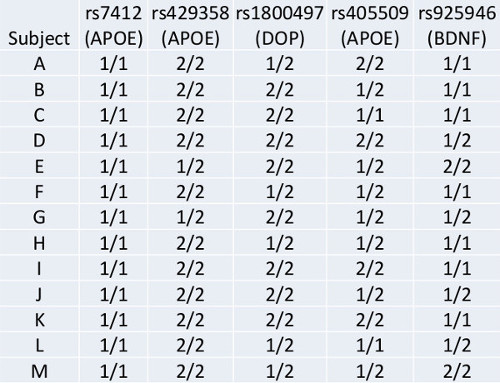
Table 3. Genetic results following PCR analysis.
