The facts that 74% of canine bone marrow samples (n=54) contained clots when they arrived in our laboratory (Figure 1A) along with decreased MSC yields from these samples, made us believe that a considerable number of MSCs was trapped within the clots. Indeed, a simple DAPI-stain of sectioned clot material confirms the presence of nucleated cells in high density (Figure 1B). This ultimately leads to low numbers of MSCs available for expansion culture, which triggered us to develop the protocol using urokinase. Typically clots disappear almost completely when applying our protocol. However, during method development we addressed the question of clot digest systematically by weighing before and after digest. These experiments revealed that the undigested remainders were 15% (dog) or 9% (human) of the initial clot weight (Figure 2A).
A typical feature of bone marrow derived MSCs is the ability to adhere to cell culture dishes. Researchers make use of this characteristic to select for MSCs. As a consequence, a colony forming assay allows to evaluate the quality of the cell pool in a simple, quantitative and reliable way. In our laboratory, the colony forming assay described herein has been applied routinely to all bone marrow samples processed (also non-clotted ones). This allowed us to use the assay as main criterion for determining the efficacy of the urokinase digest. To allow direct comparison, cells from clotted sample filtrates (i.e. as if clotted samples were just filtered but not enzymatically treated) and digested clots were seeded on separate 10 cm dishes followed by incubation for two weeks. When visualizing colony forming units (CFU) with Giemsa stain (as shown in Figure 2B), we observed 3.8 times more CFU from the urokinase reactions of canine samples than from the corresponding initial filtrates (Figure 2C). Although less prominent, human samples followed a similar trend with 1.6 fold more CFU from treated samples, confirming the suitability of the protocol. Indeed, the plates of digested clot illustrated in the right row in Figure 2B correspond to the typical result seen for a pooled sample. However, donor variation may easily result in CFU numbers from half to double of what is depicted.
Taking the colony-size as indicator of cell pool quality, more medium (2-5 mm) and large (>5 mm) colonies appeared on the plates seeded from clots compared to the CFU from filtrates (Figure 2C). This generally indicates that MSCs grow normally after urokinase treatment. Also in the aggregate, the comparison of digested canine specimens (n = 21) to samples without clot (n = 7) yielded comparable numbers of total MSCs for treated samples, although a big inter-sample variation was observed due to the heterogeneous donor population (Figure 2D).
As a last functional test of suitability, we induced differentiation of MSCs derived from digested bone marrow samples. Applications in autologous stem cell therapies are based on MSC differentiation into cartilage, bone or adipose tissue or MSC paracrine signaling 18. Cells can be guided towards the desired path of differentiation by choosing the appropriate culture conditions for adipogenic differentiation 19, osteogenic differentiation 20 or chondrogenic lineage 17. Hence, we compared MSCs from bone marrow clot to MSCs derived from unclotted bone marrow sample. After four weeks in culture, it was possible to differentiate MSCs into all three above mentioned lineages. This was histologically tested with Von Kossa (for osteogenic lineage), Oil Red O (adipogenic) and Alcian Blue (chondrogenic) stainings, showing no differences in the grade of differentiation between the groups (Figure 3).
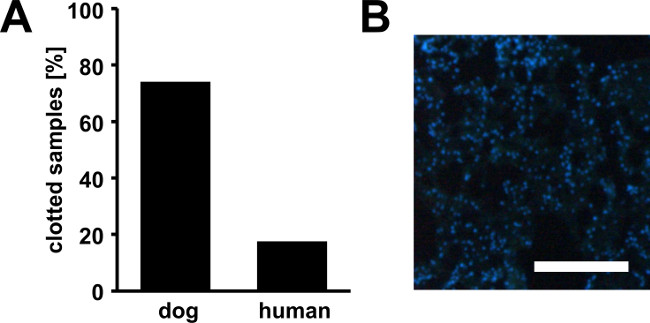
Figure 1. Bone marrow clots. Percentage of canine and human bone marrow samples in partially clotted state upon arrival (A). Furthermore, we found that MSC yields from clotted samples were strongly reduced due to a high number of cells trapped within the clots. A high number of nucleated cells are present within the clots as demonstrated by DAPI-staining of a cryosection from a canine bone marrow clot (B). Scale bar represents 200 µm.
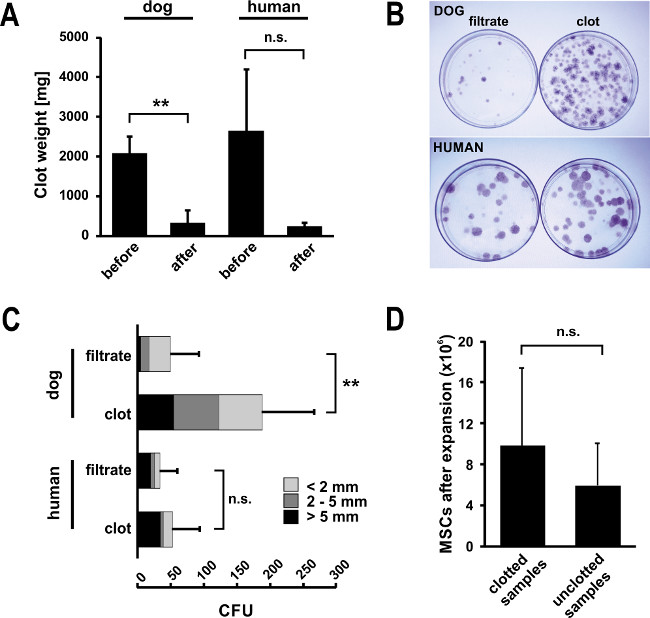
Figure 2. Isolation of MSCs from bone marrow clots digested with urokinase. (A) Typically, bone marrow clots disappear almost completely upon urokinase digest. Upon method development, we assessed clot weights for canine (n = 5, mean ± SD, **p ≤0.01) and human samples (n = 3, mean ± SD, n.s. = not significant p = 0.10) that were strongly reduced upon urokinase digest. (B) A simple CFU assay can serve as an informative tool for assessing the quality of an MSC preparation. To assess the efficacy of the digest, the CFU assay was performed for filtrates and digested clots from bone marrow aspirates separately. After two weeks in culture, 10 cm control plates were stained with GIEMSA and CFU were counted. The assay confirmed that high number of CFU can be released from the clot by urokinase digest and remain functional. This is also confirmed by the high frequency of large colonies (class-division: >5 mm in black, 2-5 mm in dark grey and <2 mm in light grey. Error bars represent SD of total CFU (n = 5 for dog, n = 3 for human, **p ≤0.01, n.s. = not significant, p = 0.17). (C) Pictures from Giemsa-stained plates confirm the results shown. The plates shown for digested clot correspond to a typical result for a digested bone marrow sample – however, numbers can vary largely due to donor variability. (D) In the sum, applying the urokinase digest protocol (n = 21) results in comparable total MSC yields after expansion culture to naturally clot free samples (n = 7, mean ± SD). Statistical analysis for the entire Figure 2 was performed using Student’s t-test.
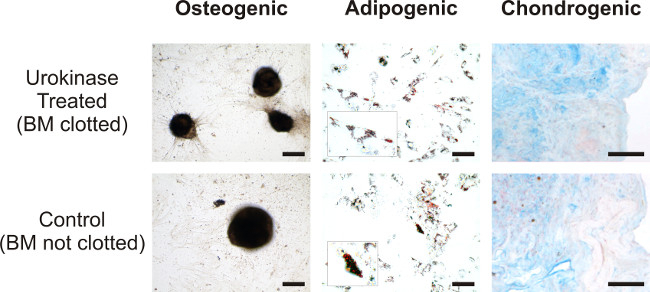
Figure 3. Comparison of differentiation potential of digested versus natively unclotted samples. Canine MSCs isolated from clotted bone marrow treated with Urokinase (top row) and unclotted bone marrow (bottom row) were differentiated in osteogenic phenotype and stained by Von Kossa (bar = 200 µm), adipogenic phenotype was stained by Oil Red O (bar =100 µm; in the insets larger magnification of fat vacuoles), while chondrogenesis was revealed by Alcian blue staining (bar =100 µm; counterstaining nuclear fast red). Please click here to view a larger version of this figure.
