Implanting an electrode into the STN of a rat using a recording system – as presented here – is an effective and accurate procedure for DBS that takes approximately 1 hr per animal. This model is a fairly minor procedure: out of 10 rats subjected to surgery, all survived the intervention. Twenty-four hr after intervention, the state of each rat was monitored and no animal achieved more than 1 of 3 points according to the severity code. During the period of continuous stimulation (14 days, 24 hr a day), no wire detached, broke or was bitten through. None of the 10 rats lost the cap of dental cement nor did they get hurt by the equipment during the phase of stimulation. The impedance measured in these 10 animals before stimulation was 353 ± 101 kΩ . Rats were stimulated at a frequency of 130 Hz and a pulse width of 60 µsec. The mean stimulus intensity was 60 µA, which was set at 20% below the intensity threshold of orofacial or contralateral forepaw dyskinesia, thereby preventing problems with feeding or locomotion during the period of stimulation.
Fourteen days after intervention and continuous stimulation, all 10 rats were euthanized by decapitation after deep anesthesia and brains were rapidly harvested. In a rat brain matrix, a 2 mm thick brain block encompassing the STN was cut and immediately frozen at –80 °C. These brain blocks were cut in coronal sections (8 µm thick). Each section was stained with hematoxylin & eosin to visualize the position where the tip of the electrode was located, as well as to detect sings of inflammation or scar tissue due to the electrode. The success rate for localizing the electrode in the STN was 8 of 10 animals. In these 8 rats, the tip of the implanted electrode was situated in the STN, as shown histologically. Figure 11 illustrates the electrode location in the STN. A small lesion developed after continuous stimulation was found in all rats. This lesion was surrounded by a small number of inflammatory cells (Figure 11).
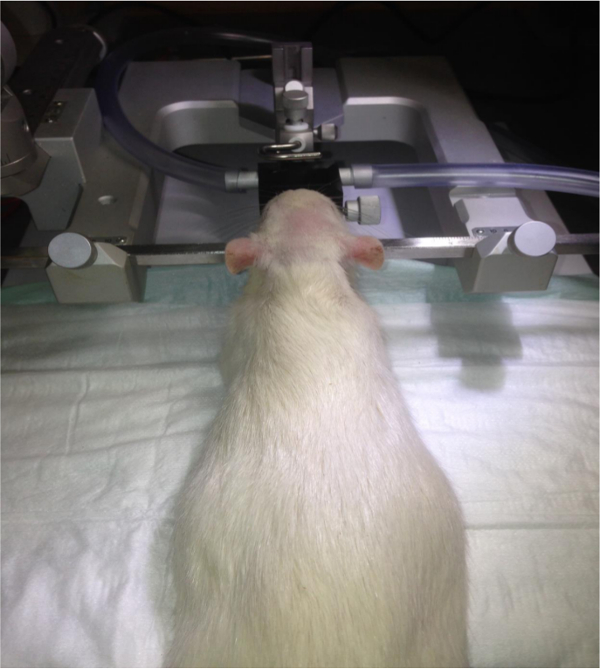
Figure 1. Fixation of the head in the stereotaxic instrument. The rat is fixed by the ear bars of the stereotaxic frame, as well as by the gas anesthesia mask. Please click here to view a larger version of this figure.
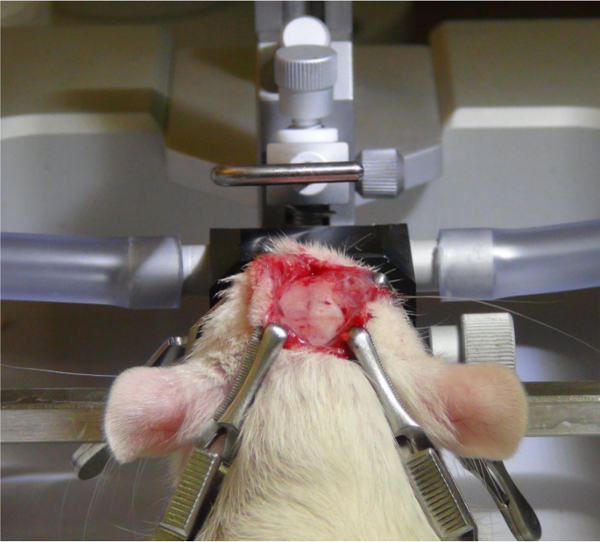
Figure 2. Exposing the skull. After a midline incision, the skin and periosteum are rolled to the wound edges and kept away from the surgical area using four clamps. Please click here to view a larger version of this figure.
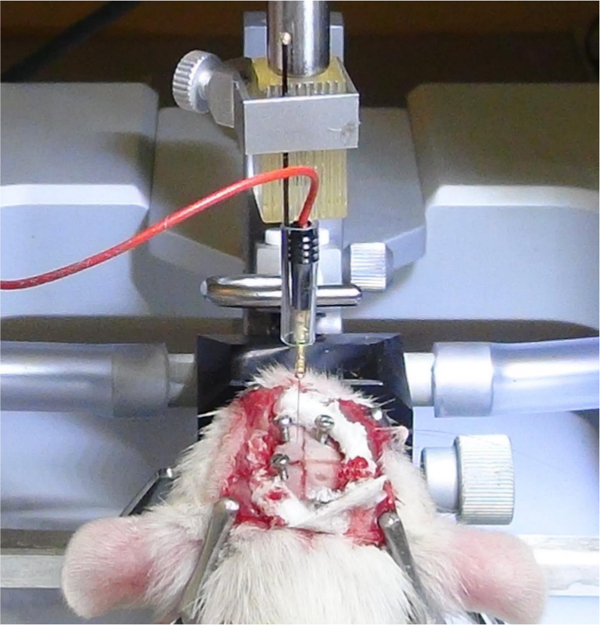
Figure 3. Fixation of the electrode in a probe holder. Using forceps, the pin of the electrode is inserted in the plug and fixed with a probe holder. The plug is connected with the recording apparatus via a wire. Please click here to view a larger version of this figure.
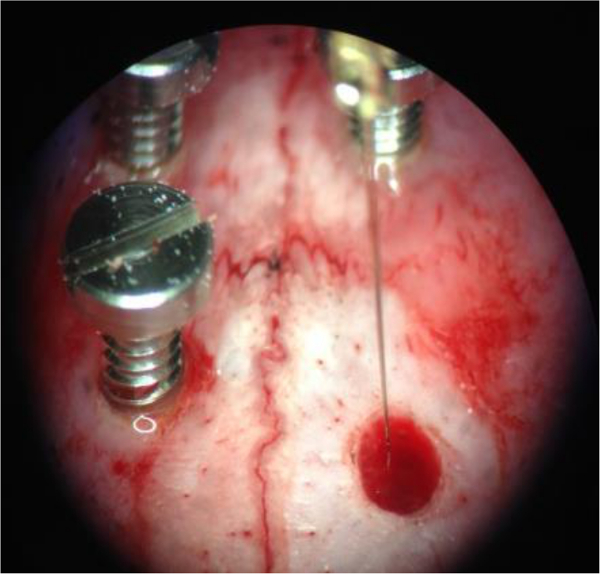
Figure 4. Insertion of the electrode in the brain. After determining the exact AP and ML coordinates of the subthalamic nucleus, the tip of the electrode is advanced to the level of the punctured dura and the dorsoventral vernier scale reading is taken. Please click here to view a larger version of this figure.
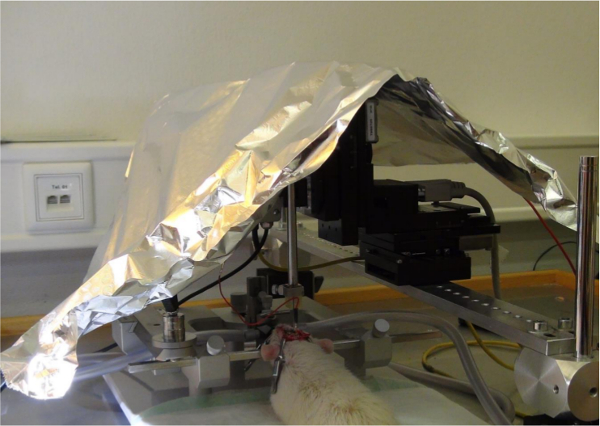
Figure 5. Protection of electric interference. A Faraday cage (or, alternatively, aluminum foil) is put over the rat in the stereotaxic instrument and the instrument, as well as the animal, is grounded. Please click here to view a larger version of this figure.
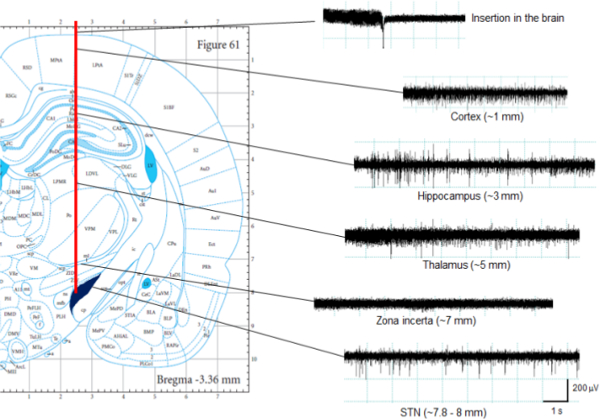
Figure 6. Recording of brain activity. The subthalamic nucleus (STN) shows an irregular firing pattern and a high firing rate (mean frequency: 40.9 ± 12.9 Hz)18. Before entering the STN, the electrode passes a relatively silent region, which is consistent with the zona incerta; the vertical size of this area measures about 0.5–1 mm. Thereafter, the number of spikes increases, indicating that the insertion into the STN is complete. Please click here to view a larger version of this figure.
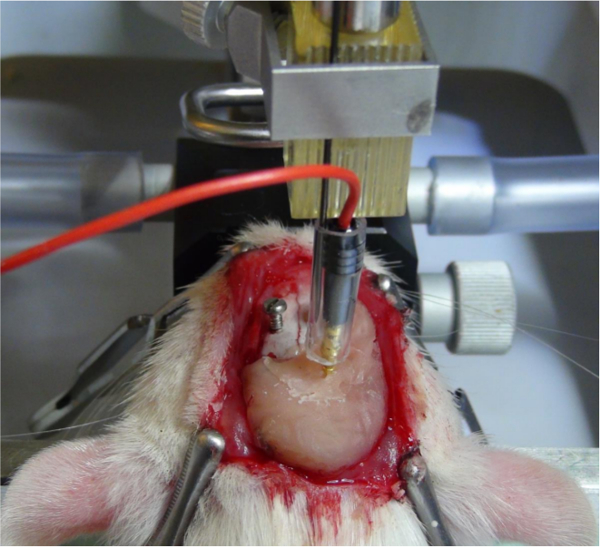
Figure 7. Fixation of the electrode. When the subthalamic nucleus is identified by means of recording, the electrode is fixed by applying dental cement around the electrode shank and the screws. This allows unplugging of the connector from the electrode pin without shifting the position of the electrode. Please click here to view a larger version of this figure.
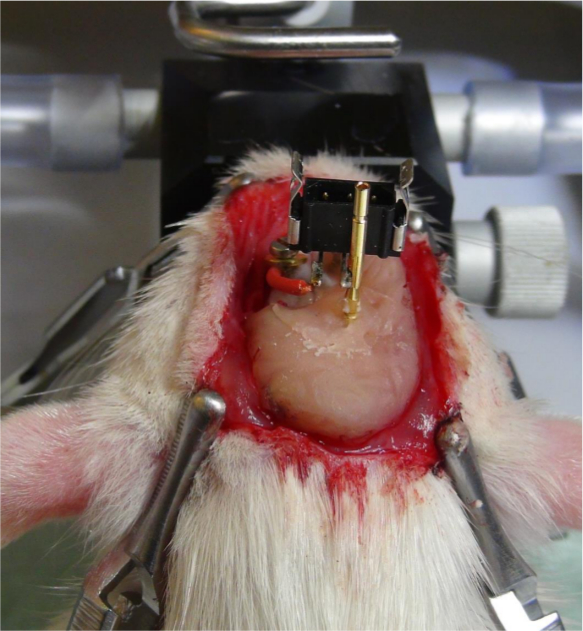
Figure 8. Attaching the plug to the electrode pin. The plug for the connector of the stimulator is attached to the electrode pin. The ground wire, which is soldered onto the plug, is fixed with a screw onto the skull. Please click here to view a larger version of this figure.
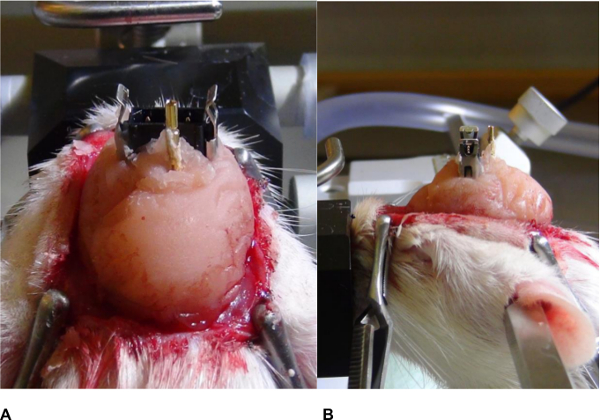
Figure 9. Fixation of the plug. (A) Frontal and (B) Lateral views. Dental cement is applied around the plug and a cap is formed; sharp edges should be avoided. Please click here to view a larger version of this figure.
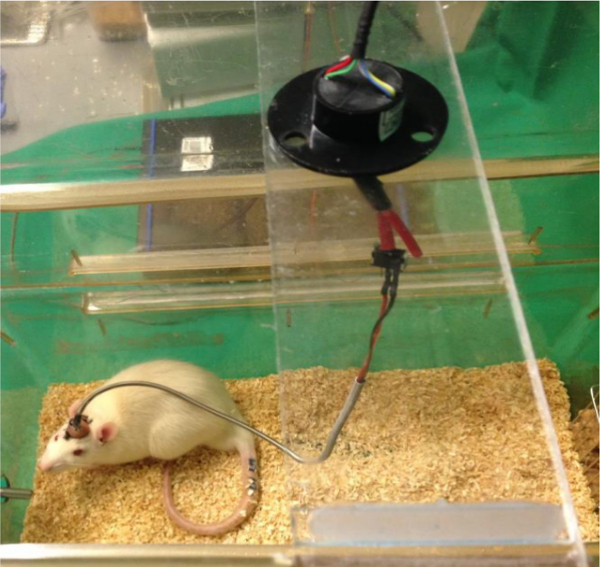
Figure 10. Connection of the rat to the stimulator. A swivel was joined into the circuit to prevent the wire from becoming tangled. A stainless-steel spring protects the wire if the rat starts to bite the wire. Please click here to view a larger version of this figure.
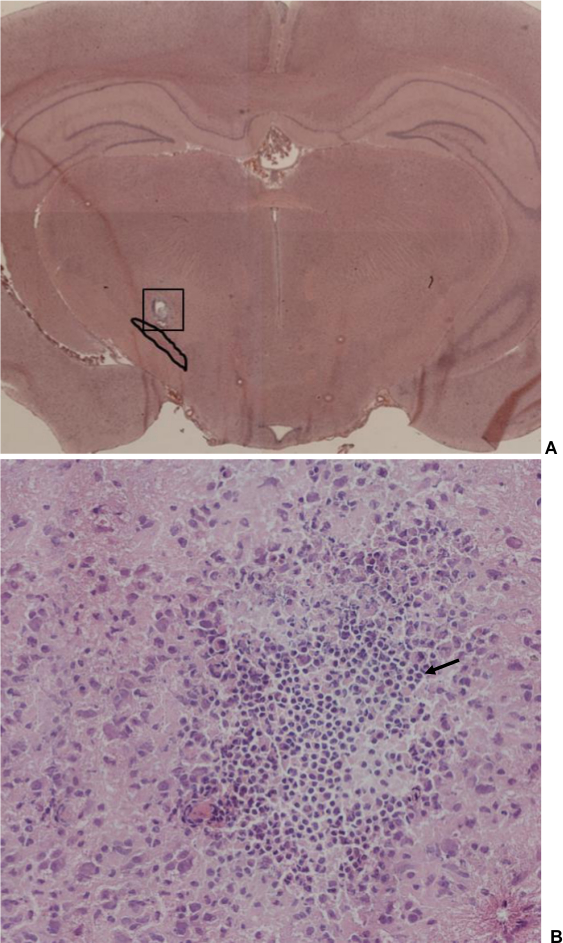
Figure 11. Brain section through the subthalamic nucleus (STN) (hematoxylin & eosin staining). (A) Overview, magnification 2.5. A solid line surrounds the STN. A small lesion is visible where the electrode tip was located during a 14 day period of stimulation. It is of note that there is no penetration canal of the electrode visible (shank diameter: 125 μm), indicating that the electrode is conserving the tissue. (B) Image detail from picture A (box), magnification 100. A small number of inflammatory cells was detectable around the lesion due to the reaction of the brain tissue to the electrode tip. Arrow: indicating an example of an inflammatory cell. Please click here to view a larger version of this figure.
