A General Method for Evaluating Deep Brain Stimulation Effects on Intravenous Methamphetamine Self-Administration
Summary
This article describes the delivery of intracranial electrical stimulation that is temporally and spatially separate from the drug-use environment for the treatment of IV methamphetamine dependence.
Abstract
Substance use disorders, particularly to methamphetamine, are devastating, relapsing diseases that disproportionally affect young people. There is a need for novel, effective and practical treatment strategies that are validated in animal models. Neuromodulation, including deep brain stimulation (DBS) therapy, refers to the use of electricity to influence pathological neuronal activity and has shown promise for psychiatric disorders, including drug dependence. DBS in clinical practice involves the continuous delivery of stimulation into brain structures using an implantable pacemaker-like system that is programmed externally by a physician to alleviate symptoms. This treatment will be limited in methamphetamine users due to challenging psychosocial situations. Electrical treatments that can be delivered intermittently, non-invasively and remotely from the drug-use setting will be more realistic. This article describes the delivery of intracranial electrical stimulation that is temporally and spatially separate from the drug-use environment for the treatment of IV methamphetamine dependence. Methamphetamine dependence is rapidly developed in rodents using an operant paradigm of intravenous (IV) self-administration that incorporates a period of extended access to drug and demonstrates both escalation of use and high motivation to obtain drug.
Introduction
Methamphetamine is a psychostimulant that produces an intense and prolonged euphoria due to an acute increase in synaptic monoamines, particularly dopamine. Methamphetamine dependence is an epidemic health problem with an estimated 25 to 34 million users globally and no proven treatment1,2. There is a substantial need to develop novel therapeutic strategies for methamphetamine dependence. Deep brain stimulation (DBS) is a neurosurgical procedure that uses a brain “pacemaker” to normalize disruptive neuronal firing patterns that occur in certain diseases, including Parkinson’s disease, dystonia, and essential tremor3. Recent human case reports suggest that DBS may also be an effective treatment for alcohol and drug dependence, but preclinical evidence regarding psychostimulants (e.g., cocaine, methamphetamine) is limited4-8.
Continuous deep brain stimulation, as it is currently practiced, requires exceptional cooperation from the patient and his/her family. Meticulous wound care and personal hygiene are required to protect the underlying pacemaker hardware, which is susceptible to infection even in patients who are not using intravenous drugs with resultant bacteremia. Regular follow-up of the DBS device is also necessary given the open loop design of the system; experienced physicians alter the settings of modern DBS to decrease target symptoms during routine clinic appointments3. This treatment paradigm will be limited in cocaine and methamphetamine users due to their challenging psychosocial situations. Several rodent studies have imitated this impractical paradigm by examining DBS effects when the therapy is delivered continuously during cocaine self-administration procedures in the drug-use environment9-11.
Non-invasive discontinuous techniques that do not require indwelling hardware, like transcranial magnetic stimulation (TMS), may be a better option for treatment of substance use disorders12. TMS is delivered non-invasively using an external headcoil to generate electrical fields in a particular brain target during daily, intermittent treatments. The recent advent of H coil or “deep” TMS allows deeper brain structures to be stimulated, in addition to cortical sites, expanding its potential use13,14. Both therapies are delivered discontinuously during a series of sessions in a different environment than that of primary drug use and have shown promise in both human and rodent trials for drug dependence13,15-17. The window to treat methamphetamine dependent patients will likely be during periods of sobriety such as court-mandated rehabilitation, not during street binges when they can experience violent or erratic behavior18. As such, the aim of this article is to describe the delivery of electrical stimulation that is temporally and spatially separate from the drug-use environment, which more closely approximates what is possible in humans, for the treatment of IV methamphetamine dependence.
Protocol
All procedures are approved by the LSUHSC Institutional Animal Care and Use Committee and were carried out in accordance with the NIH “Principles of laboratory animal care.”
1. Rodent Acclimation and Food Restriction
- Use adult Wistar rats that are 3 months old at the start of the experiment. House rats singly in cages equipped with a laminar flow unit and air filter in a temperature- and humidity-controlled, AAALAC-accredited animal care facility on a reversed 12-hr light/dark cycle (lights off at 0600 hr).
- Provide water and standard rodent chow freely until body weights are approximately 380 – 400 g. Subsequently, food-restrict rats and maintain at 85 to 90% of their free-feeding body weights during the experimental sessions to facilitate acquisition and maintenance of response to methamphetamine.
- Handle rodents in the home cage room daily from arrival throughout the experimental sessions in order to record body weight and adjust daily food allocation.
- Once target weights are achieved, prepare to surgically implant each rat with a chronic indwelling jugular catheter and intracranial stimulating electrodes.
2. Jugular Vein Catheterization
- Catheter Preparation
- Prepare a 13-cm length of silastic tubing with an inner diameter of 0.012 x 0.025', create a silicone ball 4 cm from one end of the tubing using extra silicone tubing and electrocautery, and allow to air dry.
- Dip the other end of the tubing in a limonene-based solvent derived from citrus for a few minutes and allow to expand. Connect the expanded tubing to a stainless steel guide cannula bent at a right angle.
- Anchor the bent base of the stainless steel guide cannula to a 1” square of biocompatible mesh using dental acrylic cement.
- Flush the catheter inside and out with ethanol and distilled water. Inject air through the tubing to eliminate residual liquid droplets. Allow to dry O/N.
- Sterile Technique
- Perform all surgeries in a dedicated animal surgical suite using aseptic surgical techniques. Sterilize instruments and implants using an autoclave and prepare a sterile area by placing waterproof paper on the OR table covered with a sterile towel(s).
- Wear sterile gloves and keep all instruments, implants and surgical gauze on the sterile area during the procedure. Wipe down each instrument with an alcohol swab followed by 20 sec in a bead sterilizer between procedures when multiple surgeries are performed.
- Anesthesia
- Pretreat rats with atropine (sulfate) (0.04 mg/kg, s.q.) followed by pentobarbital (20 – 50 mg/kg, ip) to achieve anesthesia.
- Inject animals with sterile penicillin G procaine suspension (75,000 units, im) and an analgesic agent (carprofen, 5 – 10 mg/kg, sc or ketoprofen, 2 – 5 mg/kg, sc) immediately prior to surgery to decrease perioperative infections and pain, respectively.
- Check for adequate anesthesia by delivering a moderate toe pinch to the animal and, if no response occurs, then proceed. Apply eye lubricant to both the eyes.
- Surgical Site Preparation
- Shave a 2 x 2 cm dorsal patch on the rat’s back just posterior to a line connecting the shoulder blades. Shave a 1 x 1 cm ventral patch in the right neck region between the jaw bone and the sternum.
- Wipe the shaved areas with alcohol pads followed by betadine solution. Place rat on a sterile towel and allow the betadine to dry before proceeding.
- Catheter Implantation
- Make an incision parallel to a line connecting the shoulder blades in the midscapular region on the back using a 10-blade knife. Use a hemostat to separate the skin from the underlying connective tissue to create a plane for the mesh catheter base. Irrigate the area with sterile saline and cover with sterile gauze prior to turning the rat onto its back.
- Make a diagonal incision between the right jaw bone and the sternum using a 10-blade knife. Use a hemostat to separate the skin from the underlying connective tissue to locate the jugular vein. Note: The jugular vein appears white/silver and shiny and is larger in male rats than in females.
- Place a spatula underneath the vein, tie a 4-0 silk suture gently around the top (proximal part) of the exposed vein and push the vein back into the neck.
- Separate the connective tissues to create a superficial pocket under the inferolateral neck skin but above the muscle. Push a sterilized trocar from the neck incision to the midscapular incision by tunneling back behind the arm and upward. Run the catheter from the back to the neck by inserting a stiff guide wire up through the trocar from the neck end and into the distal catheter. Pull the guide wire back through to the neck incision and the attached distal catheter will follow.
- Isolate the right jugular vein over a spatula by pulling up on the previously placed proximal suture. Use a ball scissors to make a small partial cut on the topside of the vein.
- Insert a curved forceps into the vein incision to open it up. Keeping the forceps apart but in place, pass the catheter tip in between the forceps tips and into the vein about 2 – 3 cm where it will terminate outside the right atrium.
- Secure the catheter by tying a 4-0 silk suture around the distal vein. Tie the proximal and distal sutures together in a “box” knot to add extra stability.
- Flush catheter with heparinized sterile saline and draw back blood to confirm successful implantation. Trim the sutures 1 – 2 mm above the knots and tuck the remaining proximal catheter under the neck skin. close with an appropriate suture/method of your choosing. If non-absorbable sutures or staples are used, they must be removed in 10-14 days under general anesthesia. Cover incision with antibiotic ointment using a sterile cotton tip applicator.
- Anchor the distal catheter/guide cannula/mesh assembly to the subcutaneous back tissue using absorbable sutures at two of the opposing corners of the mesh base. Close the back incision around the guide cannula using interrupted, non-inverted absorbable sutures. Cover incision with antibiotic ointment using a sterile cotton tip applicator.
- Postoperative Care
- Flush the catheter with heparinized 0.9% sterile saline solution using a 3 ml syringe and place an obturator into the guide cannula to prevent clogging.
- Flush each rat’s catheter on a daily basis to maintain patency.
- Immediately following the procedure, place the rat in its home cage over a heating pad in the surgical suite and observe until consciousness and spontaneous movement return.
- Return the recovered rat to the colony room and allow five to seven days to pass before intracranial surgery. Weigh, handle, and assess their general condition daily, including checking for infection and evaluating animal behavior, appearance and activity levels.
- Consult the Animal Resources veterinarian if any problems arise and follow any recommended treatment regimens. Inject animals with an analgesic agent (carprofen, 5 – 10 mg/kg, sc or ketoprofen, 2 – 5 mg/kg, sc) to treat perioperative pain as needed.
3. Intracranial Electrode Placement
- Surgical Preparation
- Perform all surgeries under sterile conditions as described in section 2.2.
- Anesthesia
- Place animal in an anesthesia induction chamber and provide isoflurance gas flow into the chamber at 1,000 – 2,000 ml/min with the vaporizer set at 5%.
- Once animal is recumbent, remove from chamber and place in nose cone on padded stereotactic operating platform. Switch gas flow from chamber to nose cone and run gas with vaporizer set at 2 – 3%.
- Adjust vaporizer as needed to maintain stable respirations and no response to stimulation during surgery.
- Inject rat with sterile penicillin G procaine suspension (75,000 units, im) and an analgesic agent (buprenorphine 0.05 to 0.5 mg/kg sc) immediately prior to surgery to decrease perioperative infections and pain, respectively.
- Check for adequate anesthesia by delivering a moderate toe pinch to the animal and, if no response occurs, then proceed. Apply eye lubricant to both the eyes.
- Surgical Site Preparation
- Shave the top of the rat’s head and place the rat in ear bars to keep its head immobile during the procedure. Wipe the shaved area with alcohol pads followed by betadine solution. Allow the betadine to dry before proceeding.
- Electrode Implantation
- Grasp the scalp between and slightly anterior to the ears with forceps and use scissors to cut across the base. This manuveur will remove a 1.5 x 1 cm area of skin over the mid-skull.
- Use a 10-blade to make a circumferential incision through the pericranium down to the skull and a curved forceps to scrape off and remove the pericranium. Irrigate the area with sterile saline, dab excess blood and saline with gauze, and allow the skull to dry completely so the bony landmarks, including the bregma, can be clearly seen.
- For bilateral surgery, mount two bipolar platinum-iridium electrodes, one into each electrode holder on either side of the stereotactic operating platform. Move the first electrode into position ~1 mm over the bregma and write down the stereotactic coordinates for the anterior-posterior (AP) and medial-lateral (ML) positions, which will be shown on the digital display. Do NOT actually touch the electrode tip to the skull because the electrode will no longer function. Repeat this procedure for the other electrode.
- Calculate the final AP and ML coordinates based on the target structure of interest. Move the electrode to this position with the tip just above the skull to obtain the initial dorsoventral (DV) coordinate on the digital display. Calculate the final DV depth based on the target structure of interest.
Note: The nucleus accumbens shell was targeted in this example given its known involvement in drug-consummatory behavior8 using the following stereotactic coordinates relative to bregma:
AP entry coordinate = [Digitally displayed coordinate at bregma] + 1.6
ML entry coordinate = [Digitally displayed coordinate at bregma] ± 2.4 for right/left
DV depth = [Digitally displayed coordinate at skull surface at AP/ML entry] – 8.5 - Mark the projected entry position of each electrode on the surface of the skull with a permanent marker. Do not bump or touch the electrode’s tip during this maneuver.
- Use a round ball diamond coated burr to drill a 1.4 mm hole at each mark. Be careful not to plunge through the skull into the intracranial vault with the high-speed drill. Use a curved forceps to puncture the dura once the skull has been drilled away.
- Use a round ball diamond coated burr to drill 0.7 mm holes in an additional four locations behind the electrode entries for placement of skull screws. Use a manual screwdriver to place four 0.8 (diameter) x 3.2 (length) mm stainless steel screws into the skull, two on each side of midline. Tightly secure these screws up to about half their length into the skull because they are the major infrastructure that will hold the cranial cap in place for the coming weeks and months.
- Carefully insert the first electrode through its burrhole into the brain to the calculated DV depth by manually turning the knob that manages the Z-coordinate of the electrode holder. Turn the knob at a rate roughly equal to 1/2 turn per second to prevent undue damage to the tip of the electrode. Ensure the electrode tip does not touch the bony edge of the burrhole when entering the brain.
- Secure the first electrode using super glue layered over the burrhole and the posterior screws, followed by dental cement. Once this construct has dried completely, remove the electrode from its holder. Repeat the insertion and cementing process for the second electrode. Apply dental cement right up to the skin edge but do not overlap with the skin because this loosens the cranial cement cap long-term.
- Postoperative Care
- Place two dust caps over the electrode pedestals to prevent clogging.
- Immediately following the procedure, place the rat in its home cage over a heating pad in the surgical suite and observe until consciousness and spontaneous movement return.
- Return the recovered rat to the colony room and allow five days to pass before starting the experiment. Weigh, handle, and assess the rats’ general condition daily, including checking for infection and evaluating animal behavior, appearance and activity levels.
- Consult the Animal Resources veterinarian if any problems arise and follow any recommended treatment regimens. Inject animals with an analgesic agent (buprenorphine 0.05 to 1 mg/kg sc) to treat perioperative pain as needed. Intracranial bleeding can be more prevalent with the use of non-steroidal pain medications (carprofen, 5 – 10 mg/kg, sc or ketoprofen, 2 – 5 mg/kg, sc) so use buprenorphine perioperatively for intracranial surgery.
4. Operant Apparatus
- Use plastic and stainless steel operant conditioning chambers contained within sound-attenuating enclosures to run the behavioral experiments.
- Outfit each enclosure with an exhaust fan to supply ventilation and white noise to mask extraneous sounds.
- Use a personal computer and a behavioral software interface system to program the procedures and collect the experimental data.
- General Set-Up
- Equip each experimental chamber with two response levers mounted on one wall of the chamber with a stimulus light located above each lever. Designate one of the levers the “active” lever so that it results in a programmed consequence when pressed.
- Program a stimulus light located directly above the active response lever to illuminate during every operant session, indicating the availability of drug.
- Have a response on the active lever result in an infusion delivery of methamphetamine (0.05 mg/kg/infusion in 100 µl 0.9% NaCl) over 2.8 sec accompanied by the house light on the opposite wall going ON for 5 sec and the stimulus light going OFF for a 30-sec timeout.
- Count responses on the active lever but they should have no scheduled consequences during the 30-sec timeout period. For completion, record responses on the inactive lever but they should have no scheduled consequences.
5. Intravenous (IV) Methamphetamine Self-Administration Procedure
- General Preparations
- Load rats into the operant chambers as quickly and calmly as possible to minimize behavioral artifacts. Attach a stainless steel spring leash to the guide cannula on the rodent’s back and to a leak-proof fluid swivel suspended above the operant chamber.
- Ensure the integrity of the connection tubing from the swivel to the 20-ml drug syringe in a motor-driven pump located outside the sound-attenuating enclosure. To do this, push the plastic connection tubing at least ¼ of an inch onto the metal swivel tip and the drug syringe needle tip until it will not slide off with moderate pulling. Counter-balance the swivel and leash assembly to permit relatively unrestrained movement of the animal.
- Conduct operant sessions at approximately the same time each day Monday through Friday.
- Acquisition
- In order to facilitate rapid acquisition of IV methamphetamine self-administration, run rats on daily 6-hr sessions for four to five consecutive days.
- Conduct these sessions on a fixed ratio FR-1 + 30 sec schedule of reinforcementduring which rats receive one infusion of IV methamphetamine for each press on the active lever followed by a 30 sec time-out (e.g., no cue or reward consequences occur with pressing of either lever). Note: This initial prolonged and “easy” access will result in the majority of rodents acquiring significant drug taking behavior in less than or equal to one week (Figure 3).
- Maintenance
- During the second week of training, run rats on daily 2-hr sessions Monday through Friday to maintain and refine IV methamphetamine self-administration.
- Conduct sessions on a fixed ratio FR-1 + 30 sec timeout schedule of reinforcement.
- Document stable, intense responding when the total number of methamphetamine presentations across each session varies less than 10% for three consecutive sessions (Figure 4) and the cumulative number of infusions across the first 30-min is greater than the cumulative number of infusions during the second 30-min (Figure 5). Note: This criterion ensures that the rats develop a drug-loading pattern at the beginning of the session that indicates addictive behavior19 and not simply casual use.
- Post-Session
- At the end of each session, disconnect the leash from the rodent’s back. Flush the catheter with 0.1 ml of 0.9% saline solution containing 800 IU streptokinase to prevent blood clots. Insert an obturator into each guide cannula to prevent clogging before returning the rats to the home cages.
- Test the patency of the catheters immediately after the end of each experimental session on Wednesdays throughout the course of the experiment.
- Prepare a 3 cc syringe, with a 22 G needle, containing heparinized bacteriostatic saline to test catheter patency. Attach one end of a 4 to 6 inch long piece of plastic tubing to the needle and the other end to the metal post of the catheter-cannula assembly on the animal’s back.
- Infuse 0.1 to 0.2 ml of saline to ensure a clear flow and then draw the syringe plunger back. If the catheter is patent, it should both flush easily and draw back blood that will be visible in the tubing. Release the plunger and infuse another 0.2 ml to flush all of the blood back through the catheter.
- If blood cannot be withdrawn, then remove the 3 cc syringe and tubing from the metal post.
- Prepare a 1 cc syringe, with a 22 G needle, containing methohexital sodium, a fast-acting anesthetic, to further test catheter patency. Attach one end of a 4 to 6 inch long piece of plastic tubing to the needle and the other end to the metal post of the catheter-cannula assembly on the animal’s back.
- Infuse 1.5 mg and quickly remove the 1 cc syringe and tubing from the metal post on the animal’s back. Reconnect the 3 cc syringe filled with heparinized bacteriostatic saline and infuse 0.1 – 0.2 ml. If the animal loses muscle tone within 3 sec, then the catheter is patent and functional.
- See the Supplemental File “Common Pitfalls” for a pitfalls section that addresses adverse reactions to methamphetamine, failure to acquire methamphetamine self-administration, and rat extraction difficulty.
6. Brain Stimulation Apparatus
- Use 10 to 12 plexi-glass boxes (12 x 18 x 18 in) (w x h x d) to run the DBS experiments. Cover each box on the outside with stiff opaque paper that covers the back and sides of the box to prevent the rats from viewing or interacting with each other. Leave the clear front panel uncovered so the examiner can view the animals during the stimulation sessions.
- Cover the tops of the boxes with a semi-permeable panel that prevents the rats from escaping while allowing airflow. Use this panel to support the commutators that are located above each box to facilitate the electrical connection between the rodent head cap and the stimulation system.
- Use a stimulation system that can deliver constant current to multiple simultaneous animals for the DBS experiments. Use a system that consists of a user programmable digital signal processor/communications interface, a stimulator, a stimulator battery pack, a channel splitter box, and the accompanying software (See Materials Sheet).
- Use custom-length cables to connect the stimulator’s channel ports to the superior electronic pedestal of each commutator. Note: The length needed will depend on the individual laboratory. These cables are outside of the animal area and do not need to be covered in stainless steel spring.
- Connect the inferior electronic pedestal of the commutator to the implanted electrode pedestal on the rodent’s head cap using 16-in cables covered with stainless steel spring. Ensure that the cables are long enough to allow free movement to every area of the enclosure without significant tension on the head cap. Note: A cable that ends roughly where the head of the rat would be when standing on all four feet is usually adequate.
- Brain Stimulation Programming
- Use a personal computer and programming software to program the stimulation parameters (e.g., waveform, frequency, pulse width, inter-stimulus delay, current amplitude) and collect the experimental data.
- Using a visual programming language, specify which functions each device will perform to meet the experimental endpoints and which data will be stored and/or projected for viewing in real-time. The commands that run this particular project are demonstrated in Figure 1.
- Specify the desired frequency, pulse width, and amplitude into the visual control panel (Figure 2) prior to the start of the experiment. Typical parameters for high frequency stimulation in rats are similar to those used in clinical human deep brain stimulation: frequency of 130 to180 Hz, pulse width of 60 to 90 msec, and current amplitude of 100 to 250 μA4,8-10. Note: A lower current is used in the rodent due to its reduced size compared to the primate.
7. Deep Brain Stimulation Procedure
- To load rats into the boxes, attach the stainless steel spring cable from the commutator to each electrode pedestal on the head cap. Test the impedance of each electrode by running 5 μA of current at a frequency of 1,000 Hz for 2 sec.
- If impedance is equal to or less than 125 KOhm, then proceed with the experiment because the electrode is able to deliver therapeutic stimulation. If the impedance is greater than 125 KOhm, consider removing the animal from the experiment because the electrode’s high resistance may truncate the current to potentially sub-therapeutic levels.
- Run the rats through one or two mock sessions for habituation during which they will be attached to the electrode cable(s) but not receiving any active therapy. Mock testing will eliminate any non-specific behavioral effects. Immediately following each mock session, transport the rats to the operant boxes for the daily 2-hr session of IV methamphetamine self-administration.
- Counter-balance rats into two groups, an active-stimulation and a sham-stimulation cohort so that the baseline drug intake is not significantly different between groups.
- Perform daily DBS sessions on the rodent cohort for 5 days during which they receive either active electrical brain stimulation or no stimulation for 3 hr depending on their group assignment. Immediately following each DBS session, transport rats to the operant boxes for the daily 2-hr session of IV methamphetamine self-administration.
- Observe animals carefully during at least a portion of each DBS session to make sure the stimulation is not causing clear alterations in animal behavior. If any abnormal behaviors occur during/after stimulation, take care to document these observations. Note: The authors have not noticed significant behavioral alterations or changes in food/water intake during the experiment described in this article.
- Alter the length of DBS treatment, the electrical parameters, and the time between the DBS session and the operant session as needed depending on the hypothesis.
Representative Results
Following placement of an IV jugular catheter and intracranial DBS electrodes, rodents can be successfully trained to self-administer IV methamphetamine after a brief recovery period. Figure 3 shows that rats will acquire and escalate methamphetamine self-administration after 2 days of extended-access to drug with an average of 168 ± 12 infusions per session by day 4.
Rats are then moved to a daily 2-hr schedule of operant training for two reasons: 1) to prevent methamphetamine toxicity and severe behavioral alterations with persistent, prolonged access and 2) to establish a relatively stable rate of responding that can be manipulated by various therapeutic interventions. Figure 4 shows that the average number of total infusions per short access session over the second week is 75 ± 8 and generally varies by less than 10% day-to-day. Figure 5 demonstrates that rats develop an increased motivation to take drug as shown by the emergence of a “front-loading” pattern of intake by day 6 of training as compared to day 1. Once this develops, the effect is largely sustained over subsequent sessions (data not shown).
Figure 6 shows that bilateral DBS delivered in the non-drug environment resulted in a marked decrease of operant IV methamphetamine self-administration on three of five days compared to the sham stimulated group. The nucleus accumbens shell was targeted given its known involvement in drug-consummatory behavior8 using the following stereotactic coordinates relative to bregma (AP + 1.6, DV – 8.5, ML ± 2.4). Stimulation parameters and duration were loosely based on previous published experience with DBS for the treatment of psychiatric disease8,20,21 but can be adjusted depending on the experimenter’s needs. Error bars are moderate and not all days reach significance indicating the range of responses that can be seen in behavioral assessments despite a clear treatment effect. Increasing the number of rats per experiment can help compensate for this natural variability. 11 animals were initially used for this experiment. One animal was euthanized for poor feeding post-operatively, one animal was excluded due to seizures, and one animal was excluded due to DBS electrode malfunction leaving us with a total of 8 animals (N = 4 Sham; N = 4 active DBS). In general starting with about 10 – 12 rats for each experiment will allow for its successful completion.
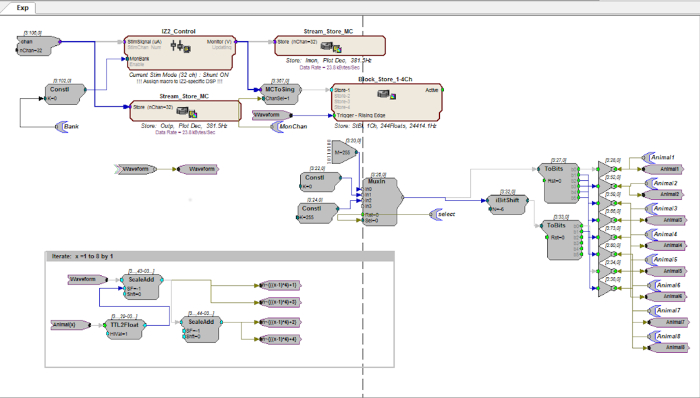
Figure 1. Visual Programming Language. The investigator uses a visual programming language, like the example shown here, to design a program that can deliver brain stimulation to multiple animals simultaneously at user-entered parameters. Please click here to view a larger version of this figure.
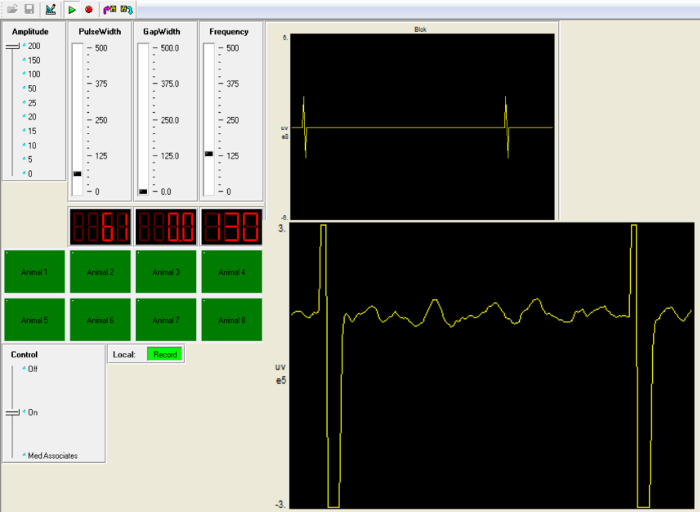
Figure 2. Visual Control Panel. Prior to the start of the experiment, the investigator specifies the desired frequency, pulse width, and amplitude on the left side of a visual control panel. Here stimulation parameters are: current intensity 200 μA; pulse width 61 msec; pulse frequency 130 Hz. Once stimulation is initiated, the waveform for the active current delivery is displayed on the right. Please click here to view a larger version of this figure.
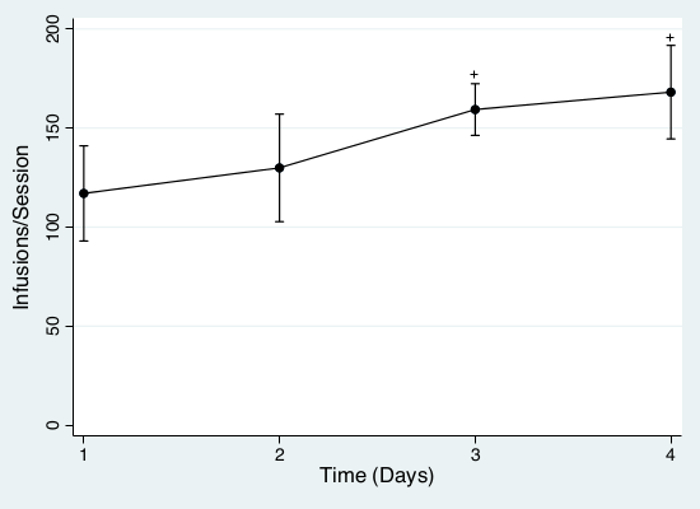
Figure 3. Acquisition of IV Methamphetamine Self-Administration. Total operant responding (360 min) data were analyzed using a repeated-measures ANOVA with the daily session defined as the repeated measure. All analyses that were p <0.05 were considered significant. Data is mean ± standard error. Total methamphetamine infusions during the daily 6-hr operant sessions over the first four days of operant training. + P <0.05 compared to sessions 1 and 2. Please click here to view a larger version of this figure.
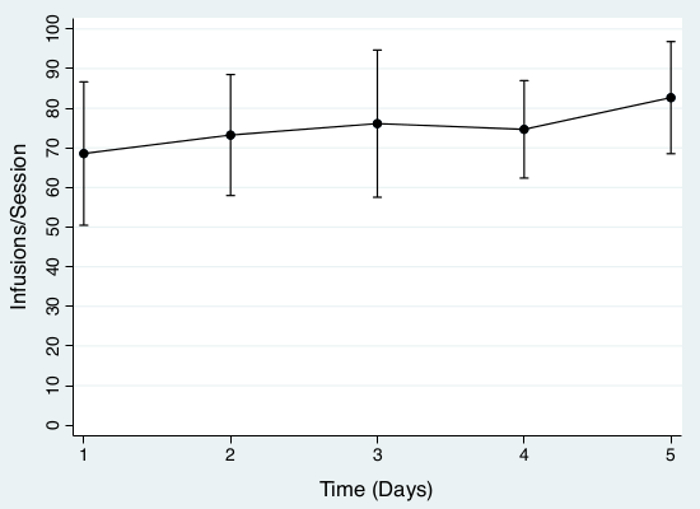
Figure 4. Maintenance of IV Methamphetamine Self-Administration. Total operant responding (120 min) data were analyzed using a repeated-measures ANOVA with the daily session defined as the repeated measure. All analyses that were p <0.05 were considered significant. Data is mean ± standard error. Total methamphetamine infusions during the daily 2-hr operant sessions over the second week of operant training, demonstrating stable but intense drug-taking behavior. Please click here to view a larger version of this figure.
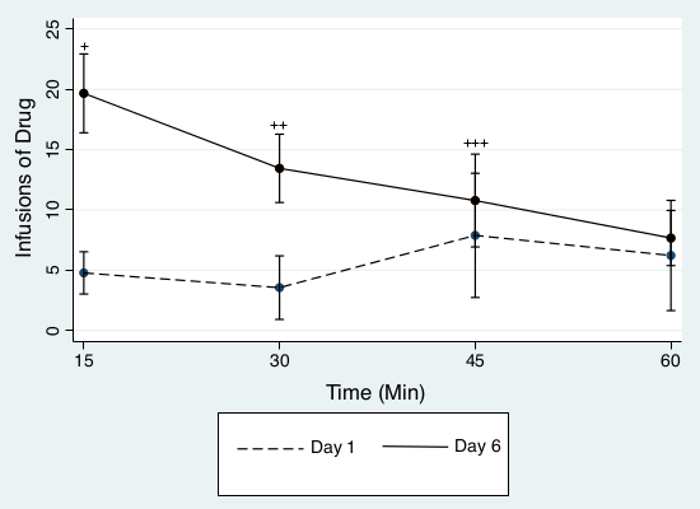
Figure 5. Development of Motivation to Take Drug. Operant responding was totaled every 15 min for the first hour and data were analyzed using a repeated-measures ANOVA with each 15-min quadrant defined as the repeated measure. All analyses that were p <0.05 were considered significant. Data is mean ± standard error. A “front-loading” pattern is not present on day 1 of operant training but develops by the second week, indicating a strong motivation to take drug. + P <0.05 compared to 30, 45, and 60 min, ++ P <0.05 compared to 45 and 60 min, +++ P <0.05 compared to 60 min. Please click here to view a larger version of this figure.
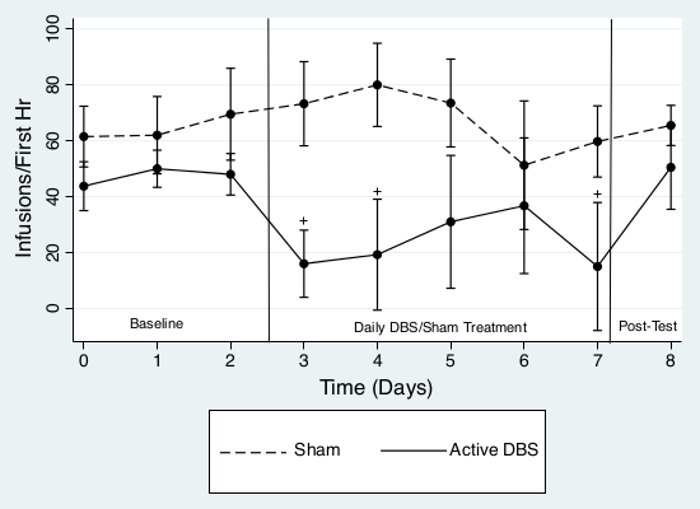
Figure 6. DBS Effects on IV Methamphetamine Self-Administration. Total operant responding in the first hour (60 min) data were analyzed using a mixed ANOVA with a between subject variable of treatment (DBS vs Sham) and a repeated measure of daily session. All analyses that were p <0.05 were considered significant. Data is mean ± standard error. Bilateral pre-operant deep brain stimulation significantly reduced the number of methamphetamine infusions over the first 60 min of operant responding on treatment days 3, 4, and 7. + P <0.05 compared to sham group and baseline responding. Responding returned to baseline levels after daily treatment ended. Please click here to view a larger version of this figure.
Discussion
Although the exact mechanisms of deep brain stimulation are not fully characterized, DBS efficacy for both motor and psychiatric disorders may result from a dynamic interaction between the electrical therapy and the functioning of various subcortical and cortical brain regions over time6,22-26. While non-contingent methods of methamphetamine delivery to rodents are well-described27,28, these methods are most appropriate for discrete investigations of drug pharmacokinetics and neurochemical effects27-29. Operant IV drug self-administration, by incorporating an element of motivation for drug, is ideally suited for the study of how electrical therapies like DBS interact with pathological behaviors over time. The procedures we describe examine the effects of DBS in one environment on contingent methamphetamine use in a different environment.
There are three key steps in our IV methamphetamine self-administration paradigm: 1) Induction of rapid acquisition and escalation of drug intake during long access sessions, 2) Maintenance of a stable, high rate of drug intake during subsequent short access sessions and 3) Development of a front loading pattern of drug taking. This paradigm can be accomplished in a 2 to 3 week timeframe with 10 – 12 rats per experiment, which is both cost-effective and ideally suited to test the effects of DBS given the potentially limited lifespan of head caps in rodents using psycho-stimulants. This procedure, like other paradigms that incorporate a period of long access19,30,31 reasonably simulates some aspects of substance use disorders; it demonstrates both escalation of use and high motivation to obtain drug with early session “drug-loading,” which are important aspects of human dependence versus recreational use19,30. Rodents who have long access exposure to IV methamphetamine also demonstrate cognitive deficits32, distinct responses to pharmacological treatment33, pharmacokinetics34 and neurochemical changes35 that are more similar to humans suffering from chronic methamphetamine use disorder than rodents with only short access exposure.
Likewise there are three key steps in our deep brain stimulation procedure: 1) Habituation to the DBS environment, including the head tether connection, for one or two “mock” sessions, 2) Daily, intermittent delivery of active stimulation using a commercial system, and 3) DBS disconnection and subsequent transport to the drug setting. This paradigm is designed to mimic the process of non-invasive therapies like TMS rather than that of traditional continuous DBS. Fully implanted, programmable DBS systems like those used for common movement disorders3 will be marginally feasible in patients suffering from psycho-stimulant dependence for several aforementioned reasons. Intermittent electrical treatment strategies that do not involve high-risk surgery and aftercare, like TMS, may be better adapted to this patient population. The methods we have described will allow investigators to develop and refine treatment strategies that can modify drug-related behavior while being delivered outside of the drug environment in a restricted timeframe. There is accumulating evidence that transient intracranial electrical stimulation that is patterned after specific neurophysiological deficits23 or combined with systemic pharmacotherapy36 exert long-lasting positive effects on psychiatric and drug-related behaviors for several weeks after the treatment has ceased.
The needs for initial excellent surgical technique and for ongoing care of multiple surgical sites during intense drug-use are the main limitations of this methodology. If either the IV catheter or the DBS electrodes become non-operational and/or infected, the rat must exit the study. Jugular catheter and intracranial electrode placements under strict sterile technique are best learned from experienced investigators prior to initiating these procedures independently.
This procedure is amenable to several modifications and future investigations, including examination of: 1) alternate stimulation parameters (e.g.,-stimulation waveform, pulse width, frequency, amplitude), 2) other potential therapeutic brain targets (e.g.,-nucleus accumbens core, medial prefrontal cortex, midbrain, habenula), 3) different DBS delivery patterns (e.g.,- daily DBS delivery, weekly DBS delivery, DBS at various intervals prior to operant sessions, DBS before acquisition), and, perhaps most exciting, 4) combinations of short-duration DBS and pharmaceutical agents that imitate optogenetic stimulation of selective pathways and exert enduring behavioral modifications36.
Divulgazioni
The authors have nothing to disclose.
Acknowledgements
Supported by the 2014-2015 Neurosurgery Research and Education Foundation (NREF) award and a 2014 Grant-In-Aid Award from Louisiana State University Shreveport School of Medicine (J.A.W.). We thank S. Harold and C.M. Keller for their invaluable technical assistance and teaching.
Materials
| Rodent operant chambers | Med Associates, Inc | ENV-008CT | Med Associates Inc. PO Box 319 St. Albans, Vermont 05478 USA Phone: (802) 527-2343 |
| Kopf Small Animal Stereotaxic Instrument with Digital Display Console | Kopf Instruments | Model 940 | Kopf Phone: 1-877-352-3275 Fax: 1-818-352-3275 Email: sales@kopfinstruments.net |
| Z-Series 3-DSP Bioamp Processor | Tucker Davis Technologies | RZ5D | Tucker-Davis Technologies 11930 Research Circle Alachua, FL 32615 USA Ph: 386-462-9622 www.tdt.com |
| Z-Series 32-Channel Stimulator | Tucker Davis Technologies | IZ2-32 | Software is accompanied by a manual that discusses how to program experiments using the OpenEx platform, which can be accessed here: http://www.tdt.com/files/manuals/OpenEx_User_Guide.pdf |
| 48 Volt LI-ION Battery Pack for IZ2 Stimulator | Tucker Davis Technologies | LZ48-200 | |
| 32-Channel Splitter Box for PZ5 | Tucker Davis Technologies | S-BOX_PZ5 | |
| OpenEx Ext Software Package for Multi-Channel Neural Recording | Tucker Davis Technologies | OpenEx | |
| Platinum-iridium stimulating electrodes | Plastics One Inc | MS303/8-B/SPC ELECT PT 2C TW .005" | Plastics One Inc P.O.Box 21465, S.W. Roanoke, VA 24018, PH 540-772-7950 |
| 2-channel cables between stimulator and commutator | Plastics One Inc | 305-441/2 W/ Spring | |
| 2-channel cables between commutator and electrode pedestal | Plastics One Inc | 305-305 W/ Spring | |
| 4-channel commutators | Plastics One Inc | SL2+2C and SL2+SC/SB |
Riferimenti
- Panenka, W. J., et al. Methamphetamine use: a comprehensive review of molecular, preclinical and clinical findings. Drug Alcohol Depend. 129, 167-179 (2013).
- United Nations Office on Drugs and Crime. . World Drug Report 2014. 14, (2014).
- Miocinovic, S., Somayajula, S., Chitnis, S., Vitek, J. L. History, applications, and mechanisms of deep brain stimulation. JAMA Neurol. 70, 163-171 (2013).
- Muller, U. J., et al. Deep brain stimulation of the nucleus accumbens for the treatment of addiction. Ann N Y Acad Sci. 1282, 119-128 (2013).
- Luigjes, J., et al. Deep brain stimulation in addiction: a review of potential brain targets. Mol Psychiatry. 17, 572-583 (2012).
- Pierce, R. C., Vassoler, F. M. Deep brain stimulation for the treatment of addiction: basic and clinical studies and potential mechanisms of action. Psychopharmacology (Berl). 229, 487-491 (2013).
- Yadid, G., Gispan, I., Lax, E. Lateral habenula deep brain stimulation for personalized treatment of drug addiction. Front Hum Neurosci. 7, 806 (2013).
- Wilden, J. A., et al. Reduced ethanol consumption by alcohol-preferring (P) rats following pharmacological silencing and deep brain stimulation of the nucleus accumbens shell. J Neurosurg. 120, 997-1005 (2014).
- Guercio, L. A., Schmidt, H. D., Pierce, R. C. Deep brain stimulation of the nucleus accumbens shell attenuates cue-induced reinstatement of both cocaine and sucrose seeking in rats. Behav Brain Res. 281, 125-130 (2015).
- Vassoler, F. M., et al. Deep brain stimulation of the nucleus accumbens shell attenuates cocaine priming-induced reinstatement of drug seeking in rats. J Neurosci. 28, 8735-8739 (2008).
- Friedman, A., et al. Electrical stimulation of the lateral habenula produces enduring inhibitory effect on cocaine seeking behavior. Neuropharmacology. 59, 452-459 (2010).
- Gorelick, D. A., Zangen, A., George, M. S. Transcranial magnetic stimulation in the treatment of substance addiction. Ann N Y Acad Sci. , (2014).
- Zangen, A. IS 44. Development and applications of deep rTMS in depression and addiction studies. Clin. Neurophysiol. 124, e53 (2013).
- Alba-Ferrara, L. M., Fernandez, F., de Erausquin, G. A. The Use of Neuromodulation in the Treatment of Cocaine Dependence. Addict Disord Their Treat. 13, 1-7 (2014).
- Alba-Ferrara, L., Fernandez, F., Salas, R., de Erausquin, G. A. Transcranial Magnetic Stimulation and Deep Brain Stimulation in the treatment of alcohol dependence. Addict Disord Their Treat. 13, 159-169 (2014).
- Amiaz, R., Levy, D., Vainiger, D., Grunhaus, L., Zangen, A. Repeated high-frequency transcranial magnetic stimulation over the dorsolateral prefrontal cortex reduces cigarette craving and consumption. Addiction. 104, 653-660 (2009).
- Levy, D., et al. Repeated electrical stimulation of reward-related brain regions affects cocaine but not ‘natural’ reinforcement. J Neurosci. 27, 14179-14189 (2007).
- McKetin, R., et al. Does methamphetamine use increase violent behaviour? Evidence from a prospective longitudinal study. Addiction. 109, 798-806 (2014).
- Ahmed, S. H., Koob, G. F. Transition from moderate to excessive drug intake: change in hedonic set point. Science. 282, 298-300 (1998).
- Hamani, C., et al. Antidepressant-like effects of medial prefrontal cortex deep brain stimulation in rats. Biol Psychiatry. 67, 117-124 (2010).
- Laver, B., Diwan, M., Nobrega, J. N., Hamani, C. Augmentative therapies do not potentiate the antidepressant-like effects of deep brain stimulation in rats. J Affect Disord. 161, 87-90 (2014).
- Pascoli, V., Turiault, M., Luscher, C. Reversal of cocaine-evoked synaptic potentiation resets drug-induced adaptive behaviour. Nature. 481, 71-75 (2012).
- Gazit, T., et al. Programmed deep brain stimulation synchronizes VTA gamma band field potential and alleviates depressive-like behavior in rats. Neuropharmacology. 91, 135-141 (2015).
- Mayberg, H. S., et al. Deep brain stimulation for treatment-resistant depression. Neuron. 45, 651-660 (2005).
- Heldmann, M., et al. Deep brain stimulation of nucleus accumbens region in alcoholism affects reward processing. PLoS One. 7, e36572 (2012).
- de Hemptinne, C., et al. Exaggerated phase-amplitude coupling in the primary motor cortex in Parkinson disease. Proc Natl Acad Sci U S A. 110, 4780-4785 (2013).
- Segal, D. S., Kuczenski, R., O’Neil, M. L., Melega, W. P., Cho, A. K. Escalating dose methamphetamine pretreatment alters the behavioral and neurochemical profiles associated with exposure to a high-dose methamphetamine binge. Neuropsychopharmacology. 28, 1730-1740 (2003).
- Kuczenski, R., Segal, D. S., Melega, W. P., Lacan, G., McCunney, S. J. Human methamphetamine pharmacokinetics simulated in the rat: behavioral and neurochemical effects of a 72-h binge. Neuropsychopharmacology. 34, 2430-2441 (2009).
- Kamei, H., et al. Repeated methamphetamine treatment impairs recognition memory through a failure of novelty-induced ERK1/2 activation in the prefrontal cortex of mice. Biol Psychiatry. 59, 75-84 (2006).
- Kitamura, O., Wee, S., Specio, S. E., Koob, G. F., Pulvirenti, L. Escalation of methamphetamine self-administration in rats: a dose-effect function. Psychopharmacology (Berl). 186, 48-53 (2006).
- Wee, S., Specio, S. E., Koob, G. F. Effects of dose and session duration on cocaine self-administration in rats. J Pharmacol Exp Ther. 320, 1134-1143 (2007).
- Rogers, J. L., De Santis, S., See, R. E. Extended methamphetamine self-administration enhances reinstatement of drug seeking and impairs novel object recognition in rats. Psychopharmacology (Berl). 199, 615-624 (2008).
- Kufahl, P. R., et al. Attenuation of methamphetamine seeking by the mGluR2/3 agonist LY379268 in rats with histories of restricted and escalated self-administration. Neuropharmacology. 66, 290-301 (2013).
- Hadamitzky, M., Markou, A., Kuczenski, R. Extended access to methamphetamine self-administration affects sensorimotor gating in rats. Behav Brain Res. 217, 386-390 (2011).
- Le Cozannet, R., Markou, A., Kuczenski, R. Extended-access, but not limited-access, methamphetamine self-administration induces behavioral and nucleus accumbens dopamine response changes in rats. Eur J Neurosci. 38, 3487-3495 (2013).
- Creed, M., Pascoli, V. J., Luscher, C. Addiction therapy. Refining deep brain stimulation to emulate optogenetic treatment of synaptic pathology. Science. 347, 659-664 (2015).
