Both ankles of 20 healthy individuals (mean age of 27.1 ± 3.9 years), 50% female, were examined. Non-weightbearing and weightbearing tests at six different degrees of knee flexion (full extension, 20°, 30°, 45°, 60°, 75°) and the Lunge Test (uncontrolled knee flexion) were conducted. A functional brace was used to control knee flexion. Measurements were performed by two investigators blinded to each other's results. Between each individual, the order of the investigators and the order of knee flexion were altered. The D'Agostino and Pearson Test revealed no normal distribution. Multiple testing was accounted for by a Bonferroni correction (p <0.004). Standard descriptive statistics, a Mann-Whitney-U-Test for differences between the sides, gender and measurement technique (non-weightbearing vs. weightbearing), and a repeated measurement ANOVA for differences between degrees of ADF were calculated. An interclass correlation coefficient (ICC; 1,1) was used to assess inter-rater reliability.
The data presented are average values of both examiners. The inter-rater reliability ranged between 0.961 to 0.992. No gender or side differences were found. Figure 3 presents the pooled data of both sides for ADF for each step of knee flexion. All weightbearing measurements resulted in significant higher ADF values compared to non-weightbearing measurements (Mann- Whitney-U-Test, p <0.001).
The boxplots presented in Figure 4 show pooled ADF differences (delta) between each step of knee flexion. Significant differences were only observed between full knee extension and 20° of knee flexion (p <0.001). Further knee flexion did not result in an increase of ADF. No significant differences for ADF were found between the Lunge test and any weightbearing examination with the knee flexed (20° to 75°).
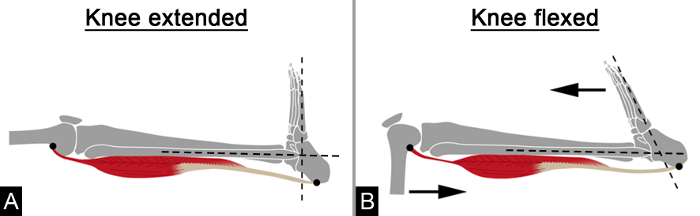
Figure 1. Schematic Illustration of the Functional Anatomy of Testing Isolated M. gastrocnemius Tightness. (A) With full extension of the knee the tensed M. gastrocnemius restrains ADF; (B) Knee flexion reduces the tension of the M. gastrocnemius and therefore increases ADF; Figure was adapted from 17. Please click here to view a larger version of this figure.
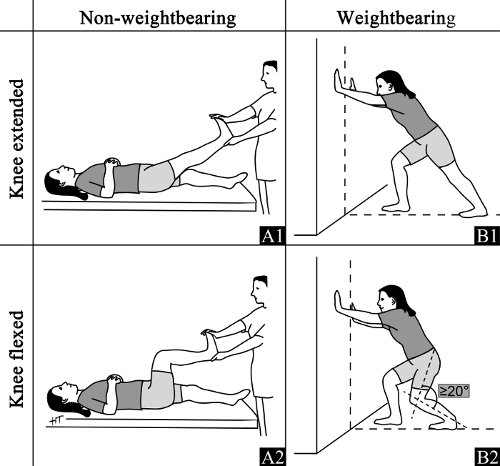
Figure 2. Schematic Illustration of the Test Procedures. (A) Non-weightbearing examination: The investigator applies force to the plantar aspect of the foot with the knee fully extended (A1) and 90° flexed (A2). The second investigator measures ADF. (B) Weightbearing examination: The subject gets into the lunge position with the rear leg centered on a line. ADF is measured with the knee fully extended (B1) and at least 20° flexed (B2). For both measurements take care that the foot measured is in a neutral pronation-supination position. Please click here to view a larger version of this figure.
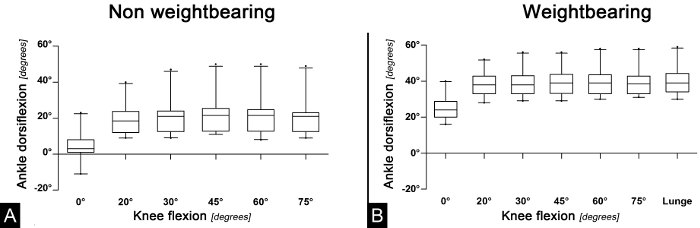
Figure 3. Boxplots (95% CI) of Pooled Ankle Dorsiflexion for Each Degree of Knee Flexion. (A) Non-weightbearing measurements: Mean ADF for each step of knee flexion; (B) Weightbearing measurements: Mean ADF for each step of knee flexion. Figure was adapted from 17. Please click here to view a larger version of this figure.
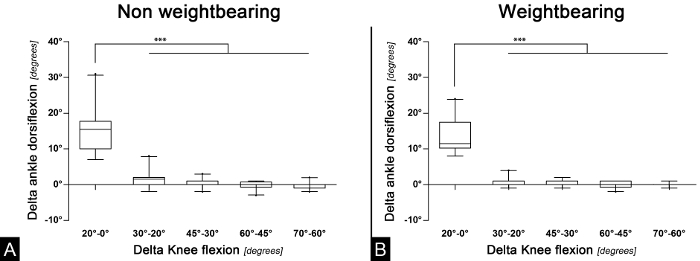
Figure 4. Boxplots of the Differences of Ankle Dorsiflexion Between Each Step of Knee Flexion (pooled values). (A) Non-weightbearing measurements: Difference of ADF between each step of knee flexion; (B) Weightbearing measurements: Difference of ADF between each step of knee flexion; ***: p <0.001; Figure was adapted from 17. Please click here to view a larger version of this figure.
