A summary of the key steps in isolating esophageal epithelial cells from patient biopsies is summarized in Figure 1. Colonies of epithelial cells will form in approximately 4-5 days and will be surrounded by fibroblast feeder cells (Figure 2A). As these colonies expand they will merge with other colonies to form larger colonies (Figure 2B). Once the cultures have become 70% confluent, they need to be expanded (Figure 2C). To ensure that fibroblasts are removed from the plate prior to removing the epithelial cells, 0.05% trypsin-EDTA is used for up to 2.5 min to remove the feeders. The absence of feeders should look similar to Figure 2D. The adherent epithelial cells are then trypsinized with 0.25% Trypsin-EDTA and replated on new irradiated feeder cells (Figure 2E).
Phenotypic characterization of these cells via qRT-PCR demonstrates upregulation of P63, a marker of progenitor cells at the end of passage 1, while still maintaining E-cadherin and TJP1 expression as compared to the initial biopsy sample. This indicates that cells have been "reprogrammed" to a more progenitor/stem-like state that are more proliferative compared to non-reprogrammed cells. When these cells are taken from the conditional reprogramming conditions and plated on normal tissue culture plates, the expression of P63 decreases and TJP1 and E-Cadherin (CDH1) increases demonstrating a shift in phenotype from progenitor cell to a more differentiated epithelial cell (Figure 3A). These cells were also analyzed at passage 1 for epithelial markers via flow cytometry and greater than 90% of the cells present from three patients were positive for EpCAM (Figure 3B). Cells were also analyzed via immunofluorescence at passages 1 and 3 to ensure the phenotype over those 3 passages was not changing. The staining demonstrates the persistence of epithelial marker E-cadherin (Figure 4A-D), progenitor marker P63 (Figure 4E-H), proliferation marker KI-67 (Figure 4I-L) and epithelial tight junction protein TJP1 (Figure 4M-P).
Lastly, a growth curve was plotted using a cell line from a non-diseased patient to evaluate the doubling time of these cells in conditional reprogramming culture. Cells were plated at 100,000 cells at day 0 and were found to be just slightly over 500,000 cells at day 4 (Figure 5). The doubling time was calculated to be approximately 36-40 h. It is expected that diseased cells will have a slower doubling time, however, every patient should be assessed separately to account for individual differences.
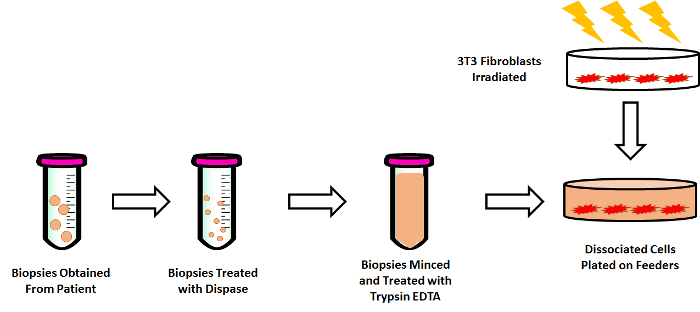
Figure 1: Overview of Isolation and Culturing Human Esophageal Epithelial Cells from Pediatric Biopsies. Biopsies are obtained from pediatric patients after informed consent and transported in keratinocyte serum-free medium to the lab. These biopsies are then treated with 1 U/ mL of dispase, followed by mincing the tissue with sterile razor blades and finally treating with 0.05% Trypsin-EDTA. The cell suspension is then added to irradiated feeder cells in conditional reprogramming medium. Please click here to view a larger version of this figure.
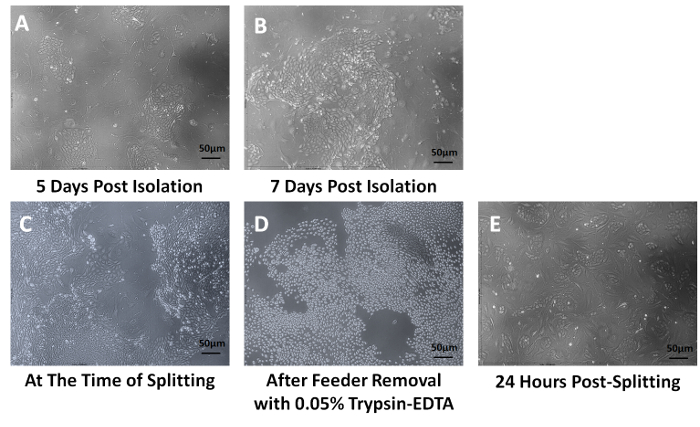
Figure 2: Culturing and Expanding Human Esophageal Epithelial Cells. After 5 days in conditional reprogramming medium, esophageal epithelial cells begin to form small cobblestone colonies (A), which eventually converge to form larger colonies (B). Once the tissue culture dish reaches 70% confluence (C), the plates are treated for a very brief time with 0.05% Trypsin-EDTA to remove the feeder cells, while still maintaining the adherence of the epithelial cells (D). The epithelial cells are then removed with 0.25% Trypsin-EDTA and replated with new feeder cells. Just 24 h after splitting these cells they will form new colonies and continue to proliferate (E). Magnification is 100X. Please click here to view a larger version of this figure.
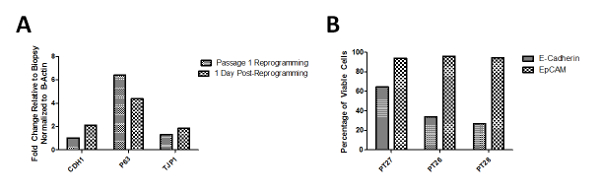
Figure 3: Flow Cytometry and qRT-PCR Analysis of Cells Expanded in Culture. (A) Representative gene expression of cells in culture at passage 1 of conditional reprogramming demonstrated a 6 fold increase in P63 expression, a marker of progenitor cells as well as a decrease in epithelial markers CDH1 and TJP1 as compared to the biopsy gene expression. This indicates the cell population is in a more progenitor-like state and therefore is more highly proliferative. Gene expression 24 h post-reprogramming (after the removal of feeder cells and ROCK Inhibitor) demonstrates increased CDH1 and TJP1 expression but a decrease in P63 expression. (B) Flow cytometry analysis of cells from multiple patients obtained at passage 1 demonstrate greater than 90% of the cells expressing EpCam. Patient 27 represents non-EoE patient cells, while Patients 26 and 28 are EoE patient cells. Please click here to view a larger version of this figure.
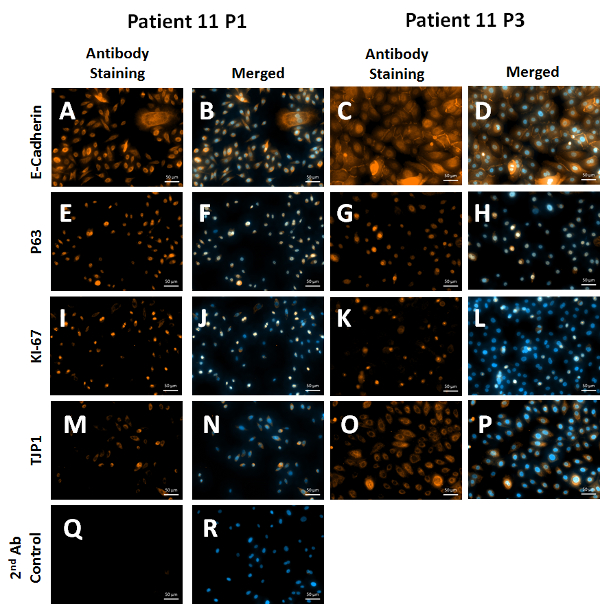
Figure 4: Immunofluorescence Staining of Cells at Passages 1 and 3. Cells grown in conditional reprogramming medium with irradiated feeder cells express E-Cadherin (A–D) as well as progenitor marker P63 (E–H). These cells are still proliferative at passage 3 (I–L). Lastly, these cells express tight junction protein 1 (TJP1), which is also consistent with an epithelial phenotype (M–P). Nuclei are counterstained with DAPI (Blue) and antibodies are detected using an Alexa Fluor 546 Antibody (Orange). 2nd Antibody (Ab) control represents non-specific binding of the secondary antibody to the tissue (Q, R). Scale bars = 50 µm. Magnification is 200X. Please click here to view a larger version of this figure.
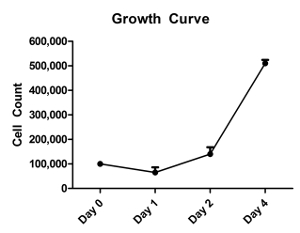
Figure 5: Growth Curve of Cells in Conditional Reprogramming. Cells in conditional reprogramming medium from a non-diseased patient were seeded at a defined density and replicates of three were counted each day for 4 days. The growth curve was generated using these cell counts and doubling time was calculated based on the numbers obtained at Day 4 and Day 0. The doubling time of these cells is approximately 36-40 h. Error bars indicate standard error. Please click here to view a larger version of this figure.
