In this manuscript, we surgically injected the murine prostate cancer cell line, Myc-CaP, into the anterior prostate lobe (Figure 1A), leading to the development of orthotopic prostate tumors with a clinically relevant TME and the correct prostate-draining lymph nodes (Figure 1B). This was performed using micro-dissecting scissors, Graefe forceps, Graefe tissue forceps, a needle holder with suture cutters, and a 50 µL syringe with a 28-gauge needle (Figure 1C). After performing an approximately 1 cm midline abdominal incision above the preputial glands (Figure 1D), one seminal vesicle and attached anterior prostate lobe were located and externalized (Figure 1E) and 30 µL (1×106 cells) of a 1:1 PBS/matrigel cell suspension was injected into the prostate (Figure 1F), as initially verified by the engorgement of the lobe and the lack of leakage (Figure 1G).
To monitor the orthotopic tumor growth, we stably transfected Myc-CaP cells to express both firefly luciferase and mCherry, allowing for tumors to be followed by non-invasive in vivo bioluminescence (Figure 2A) and fluorescence (Figure 2B), respectively. One limitation of this imaging is that, depending on the strength of the signal, imaging quantification may saturate while the tumor continues to increase in size. Therefore, with high signal intensities, this in vivo imaging is more useful for initially normalizing tumor burden across experimental groups and for later determining decreases in tumor size after experimental treatments. Additional imaging modalities can also be utilized, such as small animal MRI, PET, or CT.
Orthotopic tumors were dissected from the abdomen on day 30 after intra-prostatic injection (Figure 3A). Orthotopic tumors should be located at the site of the anterior prostate lobe. Tumor masses throughout the abdomen or attached to the anterior abdominal wall indicate improper intra-prostatic injection and leakage. With proper technique, tumor volume (Figure 3B) and weight (Figure 3C) can be recorded with relatively small standard error. However, as observed, there will be some variability with small and large tumor masses. Therefore, initial use of pre-treatment imaging quantification to equalize tumor burden between experimental arms is critical for all experiments. Further, as these murine cancer cells were injected into immunocompetent FVB/NJ mice, the TME can be analyzed by immunohistochemistry (IHC) (or flow cytometry or other techniques) for CD3 T cells (Figure 3D) (or other immune cell types). Finally, this model provides an objective survival endpoint, as the large primary tumor mass causes hemorrhagic abdominal ascites36 (Figure 3E) and/or decreased ambulation, grooming, and/or piloerection37. Occasionally, death may also be caused by tumor growth blocking urine output.
Finally, this model can be utilized to study both androgen-dependent prostate cancer and CRPC, the latter of which confers poor prognosis and is in need of novel treatment options. After orthotopic tumor development, mice were surgically castrated, as previously described38. As this is the second major survival surgery, extra care must be given to monitor for recovery and any adverse events or complications. Within 3 days after castration, strong tumor regression was observed, followed by subsequent tumor recurrence after approximately 30 days, representing CRPC (Figure 4A). CRPC tumors can be dissection and analyzed histologically, and do not display any neuroendocrine differentiation, as they maintain high AR levels and are negative for the neuroendocrine marker, synaptophysin (Figure 4B).
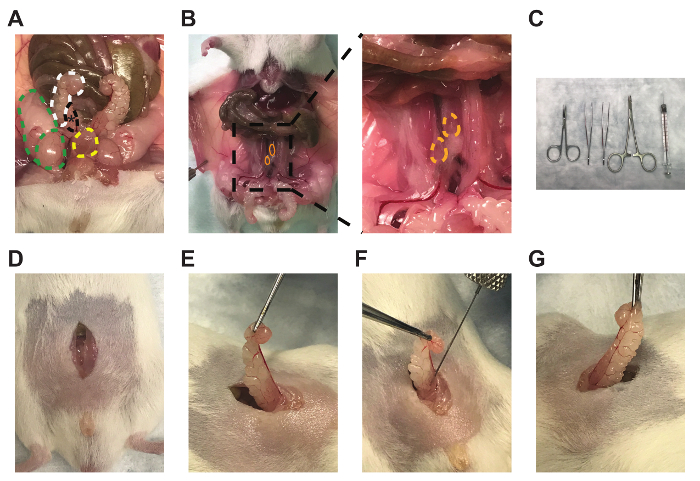
Figure 1: Anterior prostate lobe, draining lymph nodes, and representative technique for intra-prostatic cell injections. Images of the (A) right anterior prostate lobe (black, *), attached right seminal vesicle (white), right testicle and fat pad (green), and bladder (yellow), (B) bilateral prostate-draining para-aortic lymph nodes (orange), (C) micro-dissecting scissors, Graefe forceps, Graefe tissue forceps, an needle holder with suture cutters, and 50 µL syringe with 28-gauge needle (left to right), (D) midline incisions, (E) seminal vesicle and anterior prostate lobe externalization, (F), intra-prostatic injection, and (G) engorgement of the anterior prostate lobe. Please click here to view a larger version of this figure.
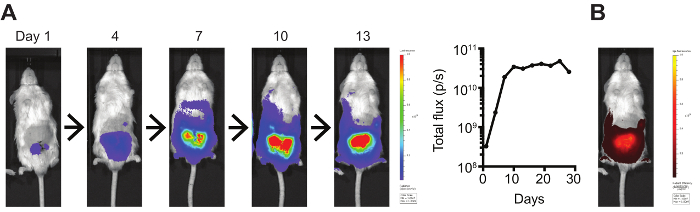
Figure 2: In vivo bioluminescent and fluorescent tumor imaging. (A) Luciferase- and (B) mCherry-expressing orthotopic Myc-CaP tumors were imaged using an IVIS Spectrum Imaging System. Bioluminescence was quantified by total flux (photons/s). Please click here to view a larger version of this figure.
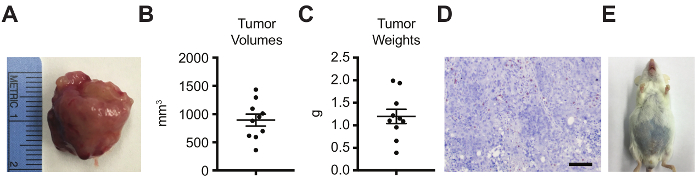
Figure 3: Orthotopic tumor analyses by tumor volume, weight, histology for immune infiltration, and survival. Orthotopic tumors were dissected on day 30 after intra-prostatic injection and analyzed by (A) gross imaging, (B) tumor volume (π/6×L×W×H; L=length of the longest axis of the tumor, W=perpendicular width, H=perpendicular height), (C) tumor weight, (D) CD3 IHC (scale bar=100 µm), and (E) survival, with the objective endpoint as the appearance of hemorrhagic abdominal ascites. (A-B) Data represented as mean ± standard error of the mean. Please click here to view a larger version of this figure.
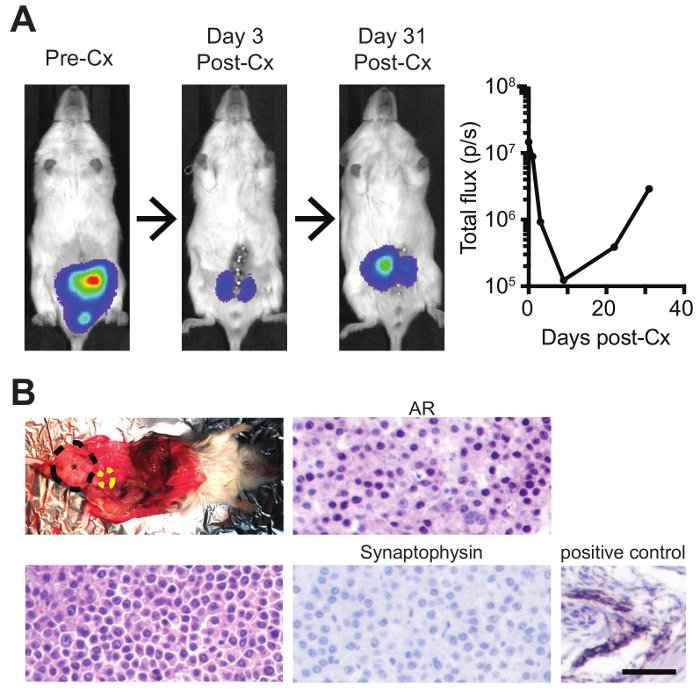
Figure 4: Intra-prostatic injections with subsequent surgical castration to model both androgen-dependent prostate cancer and CRPC. (A) Mice bearing orthotopic luciferase-expressing tumors were imaged by bioluminescence pre- and post-castration (Cx), and (B) recurred CRPC tumors were dissected (black=orthotopic prostate tumor; yellow=bladder) and analyzed by H&E, AR IHC, and synaptophysin IHC (with positive murine control) (scale bar=50 µm). Please click here to view a larger version of this figure.
