Retroductal injection can be used to administer NPs to the murine SMG (Figure 1). Here, we deliver 50 µg PSMA NPs labeled with Texas Red fluorophore.
Proper placement of the mouse allows facile access and visualization of the floor of the mouth (Figure 2A-B). The submandibular papillae are identified as two fleshy protrusions beneath the tongue. Following the cannulation (Figure 2C) and atropine injection, syringe tubing can be placed into the submandibular papillae (Figure 2D).
To facilitate the cannulation, a small puncture in the submandibular papilla is first made using the wire stylet inside of the catheter tubing (Figure 3A). Once this is done, the stylet should be retracted within the tubing to serve as a rigid guide while a larger opening is made (Figure 3B). The stylet has a diameter of 0.076 mm, while the catheter tubing has an outer diameter of 0.25 mm. Following the creation of this larger opening, the pre-loaded catheter tubing, attached to the injection syringe, can then be guided into the ductal orifice (Figure 3C).
Following the injection, it is recommended that the syringe be immobilized and injection pressure maintained. If the pressure is not applied, delivery will be successful, albeit with less efficiency and reproducibility. This is demonstrated by injecting 50 µL of 1% toluidine blue dye bilaterally and observing fainter staining in the gland without maintained pressure following the injection (Figure 4).
To verify NP delivery, the IVIS can be used to detect fluorescent signal within the mouse, which is lateralized to the injected region 1 h post administration (Figure 5). This approach enables the confirmation without euthanizing the mouse and can be continued longitudinally until signal is no longer detectable26,27.
To confirm NP persistence in the SMG 24 h following injection, glands can be sectioned, and viewed by fluorescent imaging. Aqp5 and Krt5 IHC mark secretory and ductal cells of the SMG, respectively, and show NPs in both compartments (Figure 6).
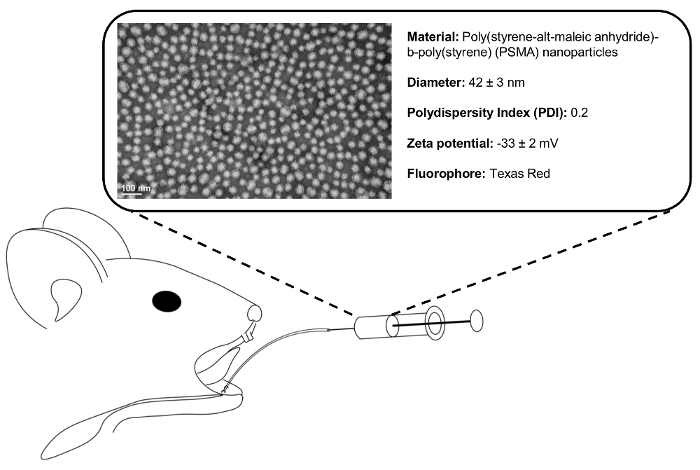
Figure 1. Retrograde injection schematic. Following ductal cannulation and syringe placement, 50 µL of 1 mg/mL polymeric NP solution is injected into the SMG. Representative transmission electron micrograph (TEM) shows monodisperse (polydispersity index = 0.2) NP population. Please click here to view a larger version of this figure.
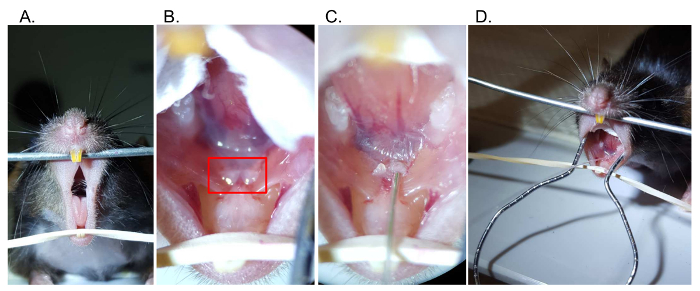
Figure 2. Retrograde injection steps. (A) Access the oral cavity by separating the maxillary and mandibular incisors. (B) Visualize the papillae (boxed) below the tongue at the floor of the mouth, which mark the location of Wharton's duct. (C) Using a catheter with wire inset, gently cannulate the base of the submandibular papilla. (D) Following cannulation, the catheter tubing can be exchanged with syringe tubing Please click here to view a larger version of this figure.
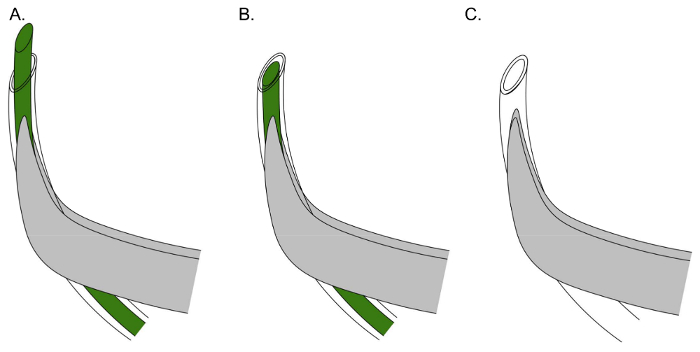
Figure 3. Effective positioning of catheter and stylet for Wharton's duct cannulation. (A) Align the tubing with the curvature of the forceps, and cut a beveled end on the tubing and wire to initially puncture the sublingual papilla. (B) Retract the stylet within the tubing to make a rigid guide to insert the tubing within the sublingual papilla. (C) Insert catheter tubing (stylet removed), joined to injection syringe, within the previously made orifice. Please click here to view a larger version of this figure.
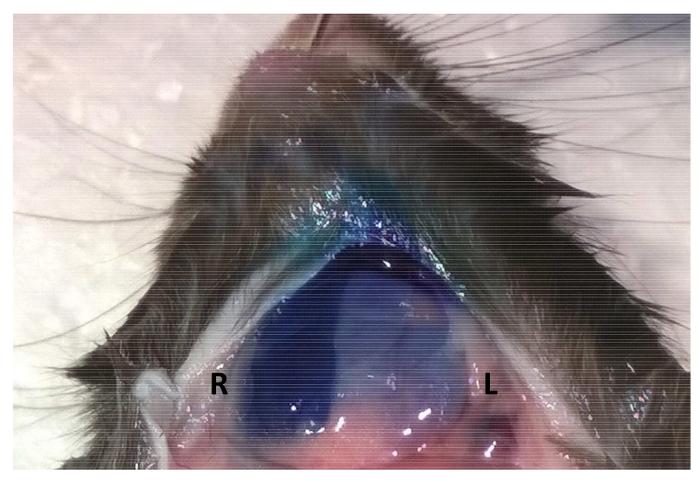
Figure 4. Maintaining syringe pressure following injection improves material retention. Following retroductal injections of 50 µL of 1% toluidine blue, syringe pressure was either maintained for 5 min (Right SMG – first injection) or the syringe was withdrawn immediately after the injection (Left SMG – second injection). Please click here to view a larger version of this figure.
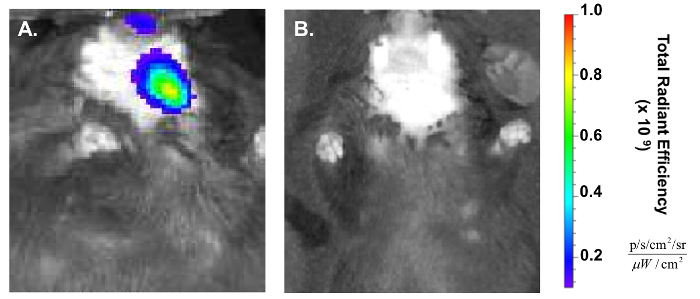
Figure 5. Confirmation of retroductal NP delivery post injection. (A) In vivo Imaging System (IVIS) shows the lateralization of red fluorescent signal to the treated (left) side of the mouse 1 h post injection. (B) NP IVIS signal at 24 h has decreased significantly. Please click here to view a larger version of this figure.
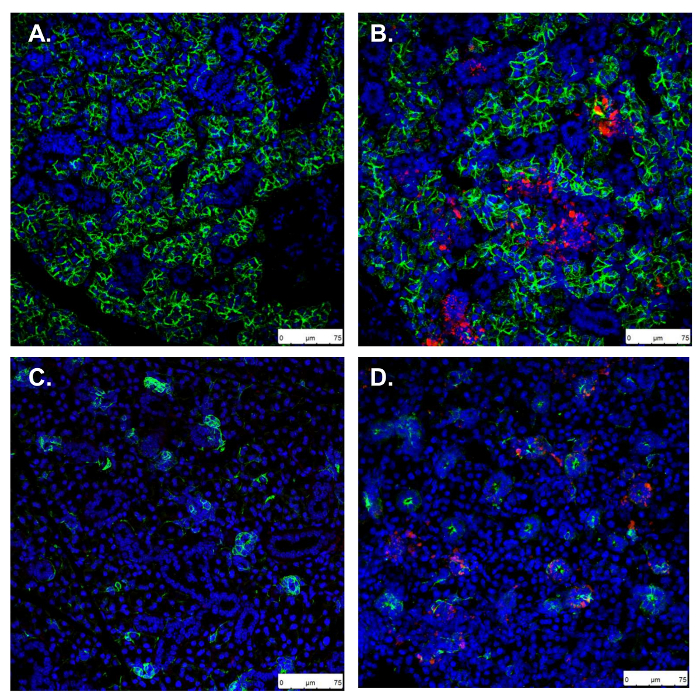
Figure 6. Confirmation of retroductal NP persistence 24 h post injection. A, C. Uninjected control SMG stained for Aqp5 and Krt5, marking secretory acinar and ductal cells, respectively. B, D. In retroductal NP injected SMG, Aqp5 and Krt5 stains show normal gland morphology and NPs taken up in both acini and ducts (scale bars: 75 µm). Please click here to view a larger version of this figure.
