Experimental chronic colitis induced by repeated administration of DSS in the drinking water is a murine model of intestinal inflammation closely resembling human IBD8,9. Figure 1 describes the effects of DSS treatment, including colon shortening (Figure 1A), a widely-used parameter to score the presence of DSS-induced inflammation, and colonic expression of pro-inflammatory genes including CXCL10, tnf and mcp-1 (Figure 1B). Infiltration of inflammatory cells was greatly enhanced by DSS treatment, showing a recruitment of the immune response in the intestinal lamina propria as analyzed by cytofluorimetry (Figure 1C).
Figure 2 depicts how colonic tissues are sectioned and inserted in the oriented cassettes. These cassettes are designed to contain a grid with extruded tips, allowing the insertion of the tissue vertically and with the proper orientation, i.e., with the lumen in the inner part and the wall exteriorly (Figure 2A, 2B, 2C). Once the cassettes are closed, the tissue orientation is preserved by the grids, contrary to what happens with conventional histological cassettes (Figure 2B).
The tissue processing is performed with an automated processor (Figure 3A–3M and Table 1), while the embedding procedure is performed with an automated embedder (Figure 4A–4M and Table 2). In the latter instrument, a robot collects the cassettes and dispenses the correct amount of paraffin. Finally, by using a microtome, sections are cut from each paraffin block. The slides are then prepared for further analysis.
Figure 5 describes the main passages of the automated H&E staining (Figure 5A–5E and Table 3) and how the slides appear after H&E staining (Figure 5F). Figure 6 and 7 show how the implementation of the automated processing and embedding protocols strongly increase the quality of the histopathological analyses of murine colonic specimens. The H&E stainings of samples prepared with the automated protocols derived from untreated mice (Figure 6A) were compared to those of DSS treated mice (Figure 6B). Histopathological scores were assessed by evaluating the modifications of different parameters occurring in the intestinal mucosa, including inflammatory cells infiltration, epithelial alterations and changes of the mucosal architecture as described in Table 4. Figure 6C depicts a representative H&E staining of a colonic tissue processed manually and included in traditional cassettes. In Figure 7, the quality of the murine tissue preparation and embedding performed through automated instruments was additionally confirmed by IHC staining of CD20 and Mallory trichrome staining8,9 in colonic sections of untreated (Figure 7A, 7C) and DSS-treated (Figure 7B, 7D) mice.
Figure 8 describes the practical relevance of this method. The same colon samples were processed and embedded either manually or through automatic methods. Each sample (either the control or DSS-treated) was cut into 2 equal parts and processed in parallel with the manual or with the automatic methods. H&E staining was then performed and a complete microscopical evaluation concerning all the pathological parameters addressing changes in the mucosal architecture, granularity, immune cell infiltrate, mucosal thickness, glandular rarefaction normally observed during intestinal inflammation, was assessed for each sample, both for the manual and automated protocol (Figure 8A and Table 4). The preparation of the samples with the automated protocol consistently allowed the evaluation of a higher proportion of histological parameters than the manual method. Additionally, a separate analysis of different histological parameters was performed (Figure 8B). The architecture and the basal infiltrate evaluation were positively affected, especially in untreated mice, by the sample preparation with the automated method.
The automated method for sample processing and embedding currently used for human histopathological analyses can be successfully applied for the analysis of murine specimens. High quality specimens are generated with the automated method that demonstrates the superiority over the manual method in the assessment of the architecture and the basal immune infiltrate of murine colonic tissues.
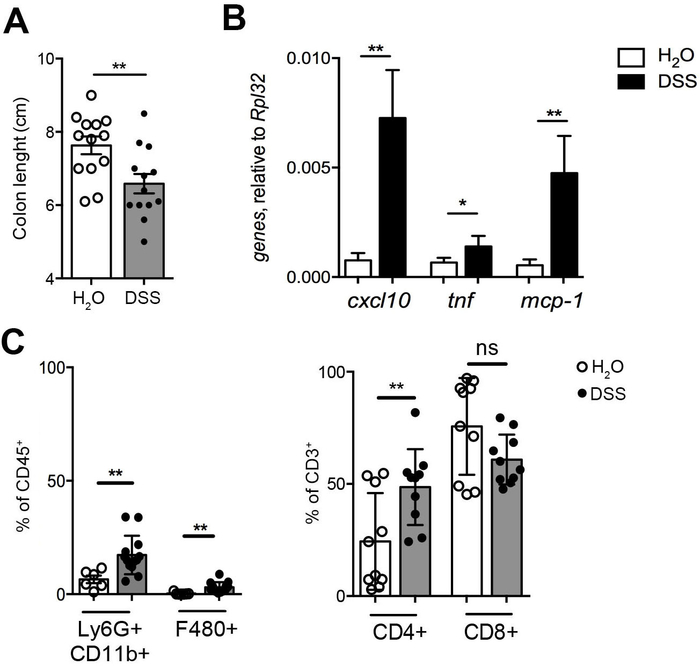
Figure 1: Chronic intestinal inflammation evaluation. (A) Colon length measurement. (B) Colonic expression of pro-inflammatory genes (cxcl10, tnf, mcp-1) in DSS-treated (black bars, n=12) and untreated mice (white bars, n=6). (C) Immunophenotyping of colonic lamina propria cells in DSS-treated (closed symbols, n=12) and untreated mice (open symbols, n=6). CD11b+Ly6G+ neutrophils, CD11b+F4/80+ macrophages (left panel), CD4+ and CD8+T cells (right panel) infiltration in controls (open symbols, n=10) and DSS-treated mice (closed symbols, n=10). Statistical significance was calculated using Wilcoxon matched-pairs signed rank t test. * p ≤ 0.05 ** p ≤ 0.01. Mean value ± SEM are reported. Please click here to view a larger version of this figure.
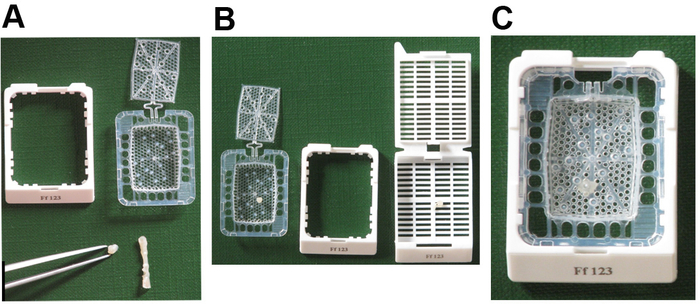
Figure 2: Description of sample preparation. (A) Instruments required for tissue preparation and picture of the orientated cassette, composed by an external cassette (white) and internal grid with extruded orientation tips. (B, C) Insertion of murine colons in the internal grids of the cassette before (B) and after (C) closure of the grids. In panel B is depicted the orientated cassette (left) or in a traditional cassette (right). Please click here to view a larger version of this figure.
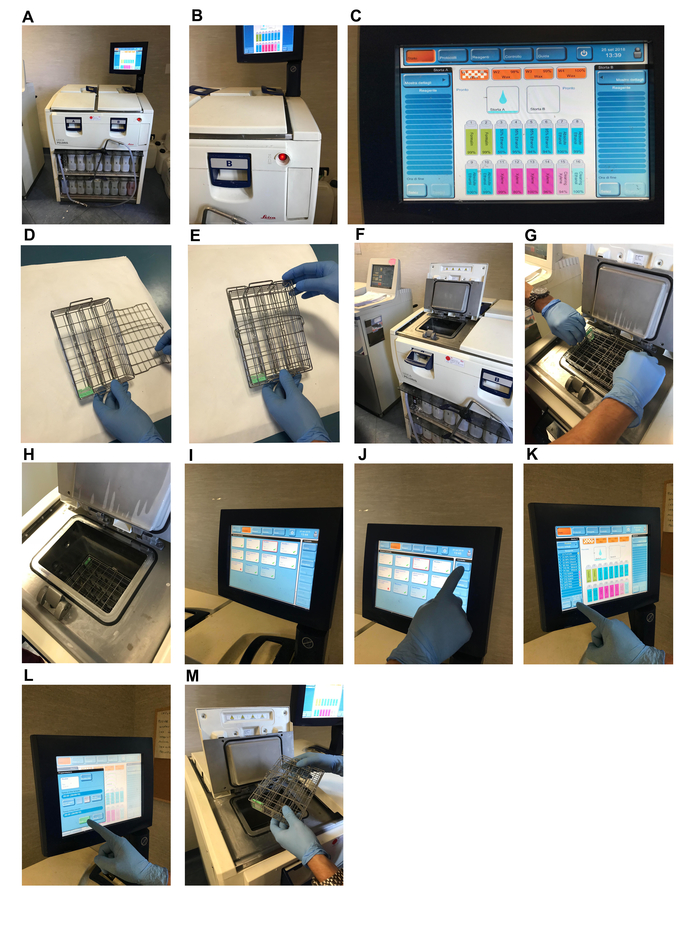
Figure 3: Description of automated processing. (A, B) automated processor. (C) Icon describing the correct paraffin wax melting temperature. (D, E) Insertion of the cassette in the metal basket (D) and its closure (E). (F, G, H) Insertion of the metal basket in the retort. (I, J, K) Selection of the processing protocol. (L) Running of the protocol. (M) Removal of the basket form the retort. Please click here to view a larger version of this figure.
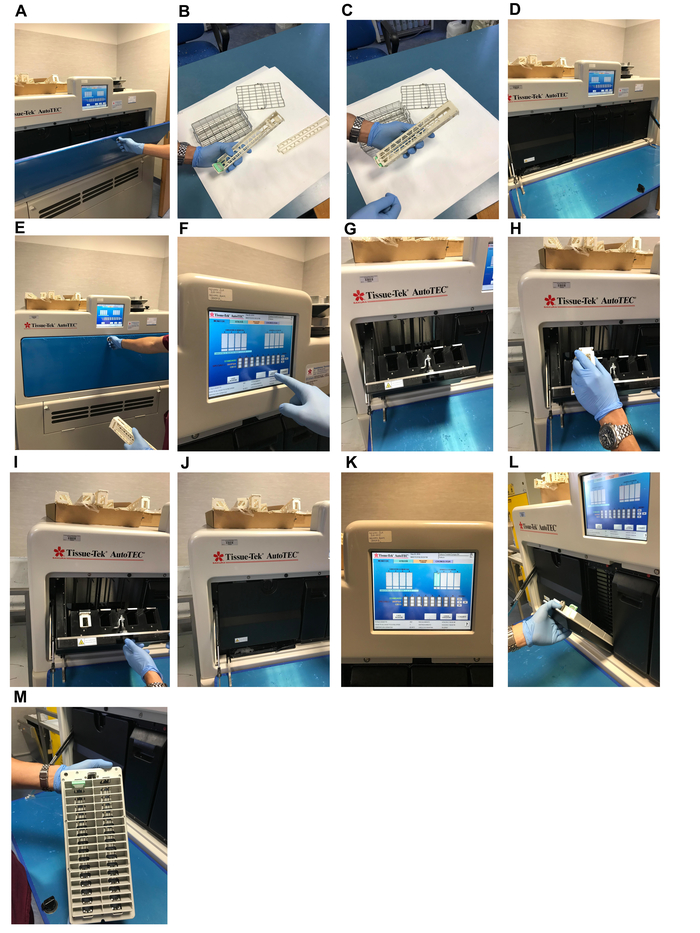
Figure 4: Description of automated embedding. (A) Picture of the automated embedder. (B, C) Insertion of the cassettes in the rack. (D, E) Opening (D) and closing (E) of the lid. (F) Signaling to the machine of the presence of a rack. (G, H) Insertion of the rack into the inlet housing. (I, J) closing of the lid. (K) Start of the embedding protocol. (L) Opening of the outlet housing lid. (M) Removal of the rack form the outlet housing. Please click here to view a larger version of this figure.
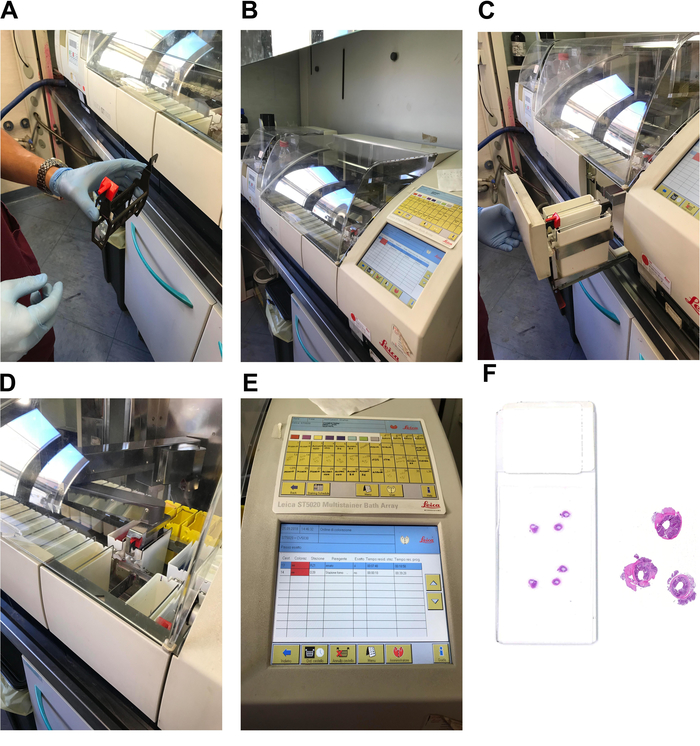
Figure 5: Description of automated H&E stainer. (A) Picture of the slide holder. (B, C) Insertion of the slide holder in the machine. (D) Closing of the machine. (E) Start of the staining protocol. (F) Exemplificative picture of a slide after microtome cutting and H&E staining. Right panel, H&E staining depicting the sample orientation. Please click here to view a larger version of this figure.
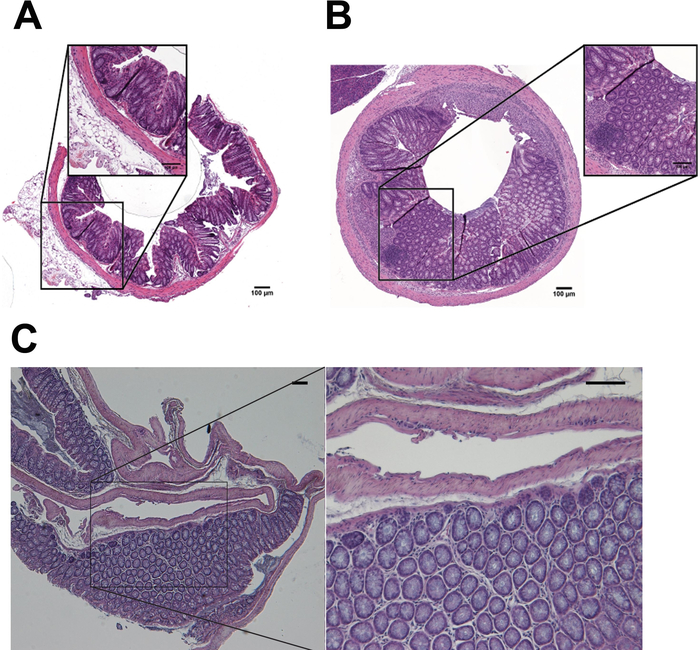
Figure 6: H&E stainings of colonic samples form untreated and DSS-treated mice. H&E staining of untreated (A) and DSS-treated (B) samples prepared (processed, embedded, stained) with automated (A, B) or manual (C) methods. Scale bar = 100 nm. Please click here to view a larger version of this figure.
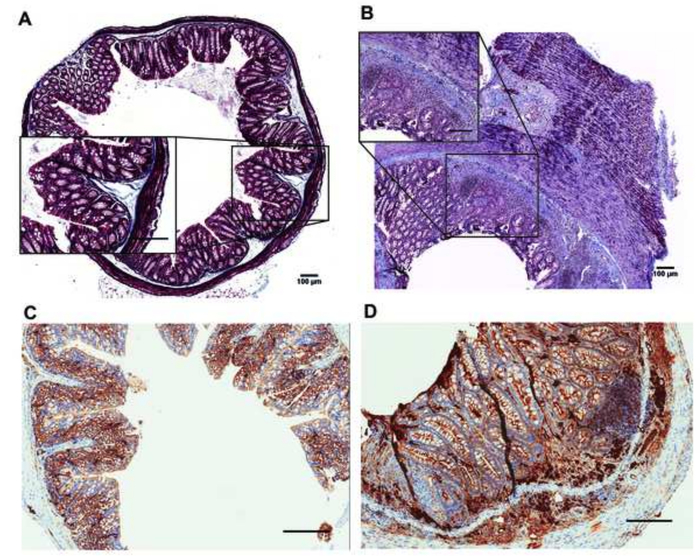
Figure 7: Mallory trichrome (A, B) and IHC stainings of infiltrating CD20+ cells (C, D) of untreated (A-C) and DSS treated (B, D) mice. Mallory staining: Blue, collagen, Dark pink, nuclei, Dark red, cytoplasm. Scale bar = 100 nm. Please click here to view a larger version of this figure.
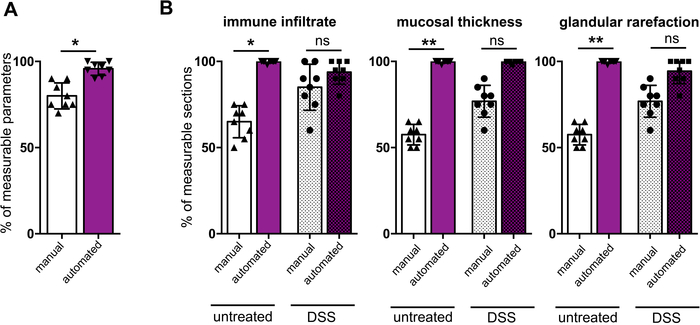
Figure 8: Comparison between histopathologic analyses with manual and automated protocols. (A) Total histopathological parameters assessable in all the sections prepared either with the manual (white bars) or with the automated method (purple bars). (B) Percentage of the indicated parameters in the samples prepared with the manual (white bars) or with the automated method (purple bars) in untreated (Plain bars) or DSS-treated mice (dotted bars). Statistical significance was calculated using Wilcoxon matched-pairs signed rank t test. * p < 0.05; **p < 0.005. Mean value ± SEM are reported. Please click here to view a larger version of this figure.
| Reagent | time (min) | temperature (°C) | pressure |
| NBF | 1 | RT | ambient |
| Ethanol 95% | 1 | RT | ambient |
| Ethanol 95% | 1 | RT | ambient |
| Ethanol 95% | 1 | RT | ambient |
| Absolute Ethanol | 1 | 45 | ambient |
| Absolute Ethanol | 11 | 45 | ambient |
| Absolute Ethanol | 30 | RT | ambient |
| Xylene | 1 | RT | ambient |
| Xylene | 1 | 45 | ambient |
| Xylene | 28 | 45 | ambient |
| Paraffin wax | 5 | 65 | vacuum |
Table 1: Automated tissue processing protocol.
| Action perfomed by the robot for each cassette |
| Remove one cassette from the rack |
| Identify the cassette |
| Pre-heat the mold |
| Place the cassette on the pre-heated mold |
| Dispense the amount of paraffin for the cassette |
| Cool down the mold |
| Allow the paraffin to solidify |
| Remove the solidified paraffin block from the mold |
| Present the block to quality sensors |
| Place the paraffin block in the output door |
Table 2: Automated embedding protocol.
| Category | Criterion | Definition | Score value |
| Inflammatory cell infiltrate | Severity (leukocyte density of lamina propria area infiltrated in evaluated hpf) | No infiltrate | 0 |
| Minimal acute (<10%) | 0.25 | ||
| Mild chronic (10-25%, scattered neutrophils) | 0.5 | ||
| Moderate chronic (26–50%) | 0.75 | ||
| Marked (>51%, dense infiltrate) | 1 | ||
| Extent (expansion of leukocyte infiltration) | Mucosal | 0.5 | |
| Mucosal and submucosal | 0.75 | ||
| Epithelial changes | Hyperplasia (increase in epithelial cell numbers in longitudinal crypts, visible as crypt elongation) | No hyperplasia | 0 |
| Minimal (<25%) | 0.25 | ||
| Mild (26–35%) | 0.5 | ||
| Moderate (36–50%, mitoses in the upper third of the crypt epithelium) | 0.75 | ||
| Marked (>51%, mitoses in crypt epithelium distant from crypt base) | 1 | ||
| Goblet cell loss (reduction of goblet cell numbers relative to baseline goblet cell numbers per crypt) | No loss | 0 | |
| Minimal (<25%) | 0.25 | ||
| Mild (26–35%) | 0.5 | ||
| Moderate (36–50%) | 0.75 | ||
| Marked (>51%) | 1 | ||
| Mucosal architecture | Ulceration (epithelial defect reaching beyond muscolaris mucosae) | No ulcers | 0 |
| Ulcers | 0.25 | ||
| Granulation tissue (connective tissue repair with new capillaries, surrounded by infiltrating cells, hypertrophied areas) | No granulation tissue | 0 | |
| Granulation tissue | 0.25 | ||
| Mucosal thickness and crypt depth | No thickening | 0 | |
| Thickening | 0.5 | ||
| Glandular rarefaction | No rarefaction | 0 | |
| Rarefaction | 0.5 | ||
| Dysplasia | No dysplasia | 0 | |
| Dysplasia | 0.5 | ||
| MAX SCORE | 6 |
Table 3: Automated staining protocol.
| Action perfomed by the stainer for each slide | Reagent | time (s) | temperature (°C) |
| Essicate | 180 | 60 | |
| Essicate | 180 | 60 | |
| Deparaffinize | Xylene | 120 | RT |
| Deparaffinize | Xylene | 120 | RT |
| Hydrate | Ethanol 96% | 120 | RT |
| Hydrate | Ethanol 96% | 120 | RT |
| Wash | Distilled wtaer | 240 | RT |
| Stain Hematoxylin | Carazzi’s Hematoxylin | 540 | RT |
| Rinse | Tap Water | 360 | RT |
| Stain Eosin | Eosin Y 1% aqueos solution | 60 | RT |
| Rinse | Tap Water | 120 | RT |
| Dehydrate | Ethanol 96% | 20 | RT |
| Dehydrate | Ethanol 96% | 20 | RT |
| Dehydrate | Absolute Ethanol | 15 | RT |
| Dehydrate | Absolute Ethanol | 15 | RT |
| Clear | Xylene | 30 | RT |
| Clear | Xylene | 30 | RT |
Table 4: Scoring scheme for the evaluation of intestinal inflammation.
