The procedures from UC collection to MSC culture are summarized in Figure 1. UC of approximately 5-10 cm in length can be collected from all newborns delivered by cesarean section. UC starts to develop at 4-8 weeks of gestation and continues to grow until 50-60 cm in length, as shown in Figure 2. There are two arteries (A), one vein (V), cord lining (CL), and Wharton's Jelly (WJ) in UC, as depicted in Figure 3 and Figure 4. UC-MSCs can be isolated from all cord regions or whole cord13. Because UC from infants with early gestational ages is fragile and difficult for dissection into a single cord region, UC-MSCs are isolated from whole cord11,12. There are several methods to isolate MSCs from UC, which include the explant method14 and enzymatic digestion method15, plus their derivatives16. Due to the longer culture cycle, lower yield, and earlier proliferation arrest associated with the explant method17,18, UC-MSCs are cultured by enzymatic digestion method as illustrated in Figure 5 and Figure 6.
The minimal criteria for defining MSCs are established by the ISCT and include their surface marker characterization19. To determine surface marker expression, UC-MSCs from preterm and term infants are incubated with appropriate PE-conjugated antibodies and analyzed by flow cytometry. They are positive for MSC signature markers (CD73, CD90, CD105) but negative for monocyte/macrophage (CD14), endothelial (CD34), hematopoietic (CD19, CD45), and major histocompatibility complex (HLA-DR) markers, as shown in Figure 7.
According to the ISCT criteria19, MSC must possess mesodermal differentiation capacity assessed by a trilineage differentiation assay. To evaluate trilineage differentiation capacity, UC-MSCs from preterm and term infants are induced to differentiate into osteocytes, adipocytes, and chondrocytes under standard in vitro differentiation conditions. As shown in Figure 8, they are well-differentiated into all three types of mesodermal cells.
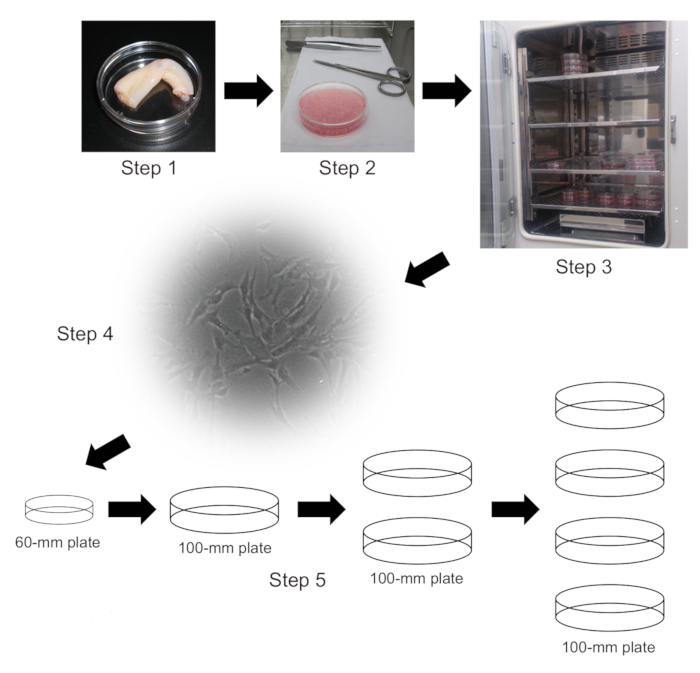
Figure 1: Schematic diagram of isolation and culture of UC-MSCs. Step 1. 5-10 cm of UC aseptically collected from placental tissue. Step 2. Purified enzyme blend-digested UC pieces. Step 3. Culture of UC-MSCs at 37 °C in a 5% CO2 incubator. Step 4. Attached UC-MSCs appeared at 3 days after initial plating. Step 5. Subculture of UC-MSCs. Please click here to view a larger version of this figure.
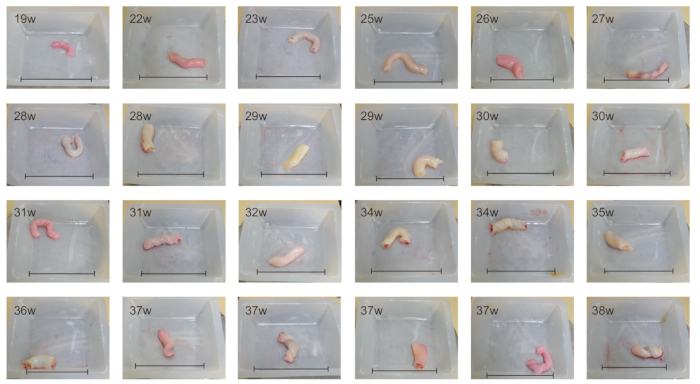
Figure 2: UC from fetuses/infants delivered at various gestational ages. UCs from fetuses/infants at 19-38 weeks of gestation are shown. The size of UC increases with gestational age. Scale bars = 8 cm. Please click here to view a larger version of this figure.
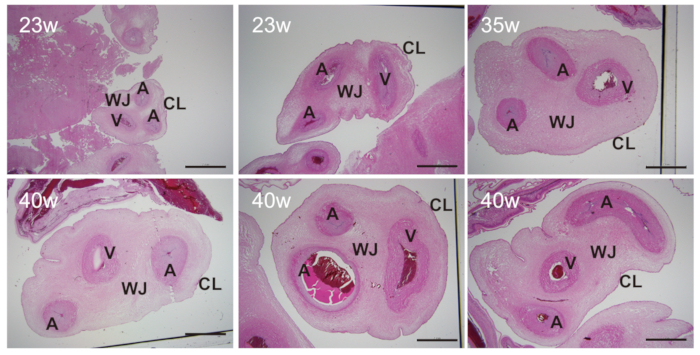
Figure 3: Sectional view of UC from preterm and term infants. There are two arteries (A), one vein (V), cord lining (CL), and Wharton's Jelly (WJ) in UC from preterm and term infants. The sizes of these tissues vary with gestational ages. Scale bars = 2 mm. Please click here to view a larger version of this figure.
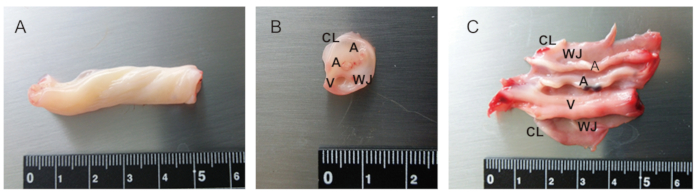
Figure 4: Anatomy of UC. (A) 5 cm of UC from term infant. (B) Cross section of UC. (C) Partially dissected UC. There are two arteries (A), one vein (V), cord lining (CL), and Whalton's Jelly (WJ). UC from infants of earlier gestational ages is particularly fragile and difficult to be dissected. Please click here to view a larger version of this figure.
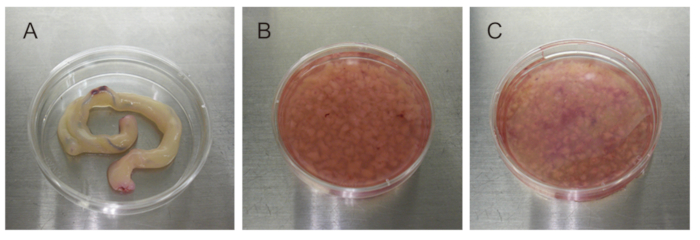
Figure 5: UC dissection using purified enzyme blends. (A) 5-10 cm of UC. (B) 2-3 mm pieces of UC. (C) Purified enzyme blend-digested UC pieces. Please click here to view a larger version of this figure.
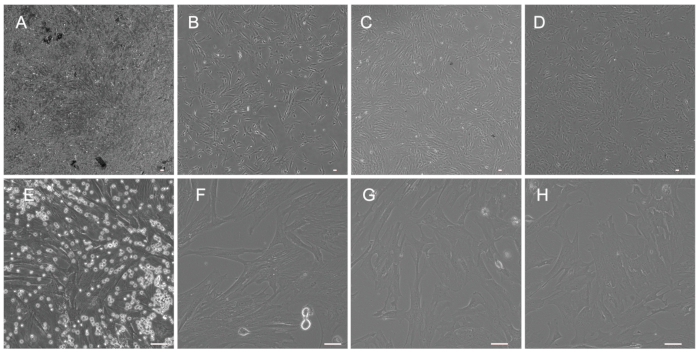
Figure 6: Morphology of UC-MSCs from preterm and term infants. (A and E) UC-MSCs at passage number 1 (P1) before the replacement of culture medium (A: X40; E: X200). (B and F) UC-MSCs at P1 after the replacement of culture medium (B: X40; F: X200). (C and G) UC-MSCs at P3 (C: X40; G: X200). (D and H) UC-MSCs at P5 (D: X40; H: X200). Scale bars = 50 µm. Please click here to view a larger version of this figure.
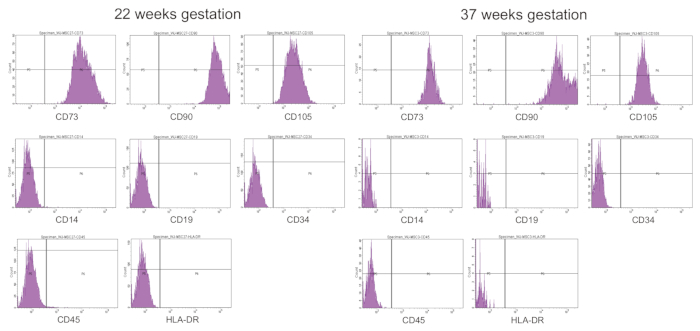
Figure 7: Surface marker expression of UC-MSCs from preterm and term infants. CD73/CD90/CD105-positive and CD14/CD19/CD34/CD45/HLA-DR-negative phenotypes are found in UC-MSCs from both preterm (22 weeks gestation) and term (37 weeks gestation) infants. Please click here to view a larger version of this figure.
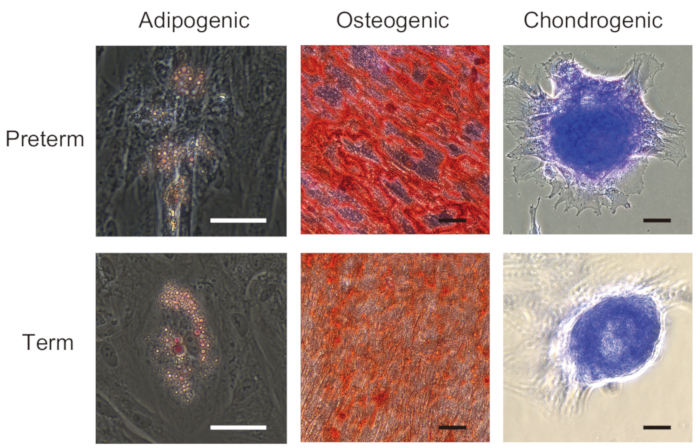
Figure 8: Trilineage mesenchymal differentiation of UC-MSCs from preterm and term infants. UC-MSCs from preterm (22 weeks gestation) and term (37-40 weeks gestation) infants are differentiated into adipocyte (visualized by oil red O), osteocyte (visualized by alizarin red S), and chondrocyte (visualized by toluidine blue). Images were taken at 200x. Scale bars = 50 µm. A part of this figure has been adapted from Iwatani et al.11. Please click here to view a larger version of this figure.
