Between 2009 and 2015, 1,042 men underwent MRI/US fusion biopsy at UCLA for either elevated PSA, abnormal digital rectal exam, or for confirmation of low-risk prostate cancer in patients considering active surveillance. Subjects underwent mpMRI of the prostate with a 3 Tesla magnet prior to biopsy. ROIs were graded on a 1−5 Likert scoring system based on suspicion of malignancy that was developed at UCLA prior to the establishment of PI-RADS. Similar to PI-RADS, the UCLA score is based on T2-weighted imaging, DWI, and DCE. Regions graded as "1" had normal T2-weighted imaging, normal DCE, and ADC on DWI of >1.2 x 10-3 mm2/s, while regions graded as "5" had a dark nodule with mass effect on T2-weighted imaging, profoundly abnormal DCE, and ADC on DWI of <0.6 x 10-3 mm2/s.
Following mpMRI, the MRI images were transferred to the fusion biopsy system's contouring software in which ROI contouring was performed, and then sent to the MRI/US fusion biopsy device. This system was used to obtain targeted cores from ROIs (if present). All patients underwent a 12-core systematic biopsy using a template generated by the fusion system regardless of whether targeted biopsy was performed. All sextants were sampled during systematic biopsy, including those that contained ROIs. The primary outcome was the detection of clinically significant prostate cancer, defined as Gleason score ≥7. The detection of clinically significant prostate cancer was compared between the different fusion biopsy strategies in patients with at least 1 ROI of ≥ grade 3. The biopsy strategies compared were targeted biopsy, systematic biopsy, and the simultaneous performance of both targeted and systematic biopsy within the same session, known as the "combination biopsy."
Figure 3 demonstrates the performance of combination biopsy compared to targeted biopsy and systematic biopsy. Among all patients, 825 patients had at least one ROI classified as grade 3 or higher. For maximum ROI grade, 435 patients had a grade 3 lesion, 301 had a grade 4 lesion, and 89 had a grade 5 lesion. Among the 825 patients with an ROI ≥ grade 3, combination biopsy had the greatest detection rate for clinically significant cancer. While 289 cases of clinically significant disease were detected via combination biopsy, 229 patients with clinically significant disease were identified using targeted biopsy alone and 199 were identified with systematic biopsy alone. Combination biopsy also identified a greater number of high-risk (≥Gleason 8) prostate cancer cases, with 89 high-risk cases diagnosed with combination biopsy compared to 74 via targeted biopsy alone (p < 0.001) and 51 with systematic biopsy alone (p < 0.001). Of this group, 15 patients with high-risk disease would have otherwise been undiagnosed if only targeted biopsy was performed.
The identification of clinically significant prostate cancer was directly related to ROI grade. 80% of men with a grade 5 ROI had Gleason ≥7 disease compared to 24% for men with grade 3 ROI. Combination biopsy also outperformed both targeted biopsy and systematic biopsy for all grades of ROI (Figure 4).
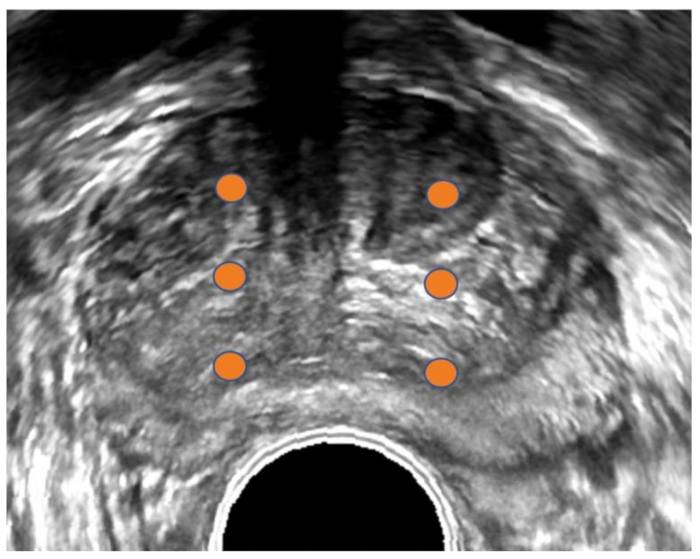
Figure 1: Transrectal ultrasound image of prostate. Conventional transrectal ultrasound (TRUS) image of prostate in transverse orientation. Orange dots demarcate sextant biopsy plan. The TRUS method is usually blind to tumor location since most tumors are not visible on ultrasound. Please click here to view a larger version of this figure.

Figure 2: 3D reconstruction of prostate. 3D reconstruction of the prostate (upper panel) and MRI with visible region of interest (ROI) shown in transverse, sagittal, and coronal views (lower panels). The ROI is shown in green (upper) and contoured in green (lower). Cores positive for malignancy are shown in red. Other cores shown in blue are negative, making this patient a possible candidate for focal therapy. Please click here to view a larger version of this figure.
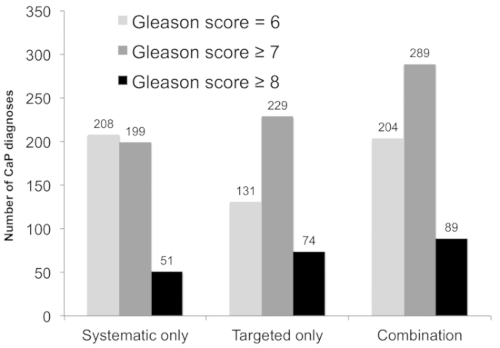
Figure 3: Diagnostic performance of systematic biopsy, targeted biopsy, and combined approach among patients whose mpMRI revealed at least one ROI of grade ≥3 (n = 825). The number of patients diagnosed with prostate cancer (CaP; y-axis) versus the biopsy strategy (x-axis) is shown. Combining targeted and systematic biopsies resulted in the detection of 60 clinically significant cancers undetected by either alone (light gray, p < 0.001 versus systematic and targeted alone), and an additional 15 high-risk cases (black, p < 0.001 versus systematic and targeted approach). This figure is adapted with permission from Filson et al.19. Please click here to view a larger version of this figure.
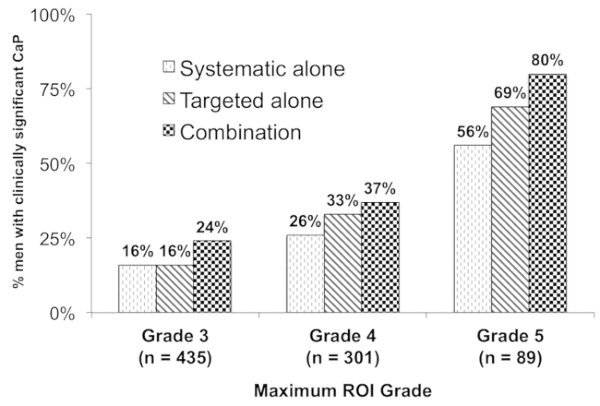
Figure 4: Relationship between the ROI grade and presence of cancer. This figure shows the proportion of patients with ≥1 ROI on MRI (n = 825) with a diagnosis of clinically significant CaP (n = 289, 35%) (y-axis) stratified by ROI grade (x-axis). Combination biopsy (black checked bars) outperformed systematic biopsy (dark diagonal bars) and targeted biopsy (light hatched bars) across all ROI grades (p < 0.001). Overall, 80% of patients with a grade 5 ROI had clinically significant CaP (versus 24% grade 3 ROI, odds ratio 9.05, 95% confidence interval 4.96–16.50). This figure is adapted with permission from Filson et al.19. Please click here to view a larger version of this figure.
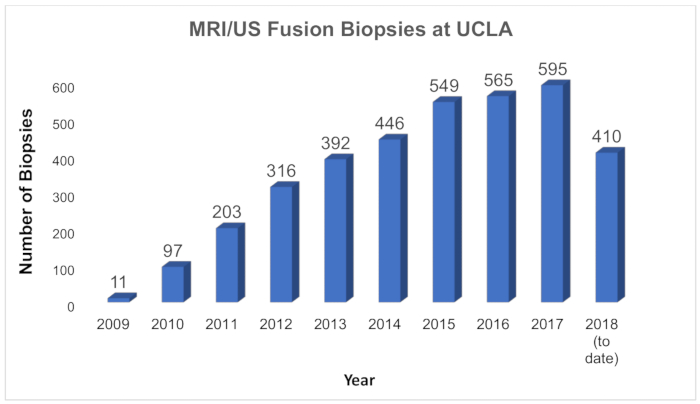
Figure 5: Growth of MRI/US fusion biopsies at UCLA. Chart showing the number of MRI/US fusion biopsies performed annually at UCLA since inception of the program in 2009. At UCLA, the new technology is used for first-time biopsy, for repeat biopsy, and serially for men in active surveillance. Please click here to view a larger version of this figure.
| Artemis (Eigen, USA) |
Position-Encoded Joints on Robotic Arm | In/out and rotational movement only (fixed to mechanical arm) | Transrectal | Robotic arm minimizes human error Training required to learn software and manual manipulation of TRUS biopsy via mechanical arm |
| BioJet (GeoScan Medical, USA) |
Position-Encoded Joints on Robotic Arm | In/out and rotational movement only | Transrectal or transperineal | TRUS-probe mounted to angle-sensing mechanical arm that exports information on probe position to workstation. |
| BiopSee (Pi Medical, Greece) |
Position-Encoded Joints on Robotic Arm | In/out and rotational movement only (fixed to mechanical arm) | Transperineal | Biopsy setup similar to brachytherapy; Diagnostic setup can potentially be used for treatment setup. TRUS probe guides transperineal biopsies |
| Real-Time Virtual Sonography (Hitachi, Japan) | Electromagnetic Field Generator for co-registration of MRI and US images | Freely movable by hand | Transrectal or transperineal | Primarily used in Japan; little studied elsewhere |
| UroNav (Invivo, USA) |
Electromagnetic Field Generator for co-registration of MRI and US images | Freely movable by hand | Transrectal | First office-based fusion platform on market Familiar freehand TRUS approach |
| Urostation (Koelis, France) | Software image-based tracking (3D US volume elastically fused to 3D MR image in real time) |
Freely movable by hand | Transrectal | Most common platform in Europe Relies purely on 3D TRUS image tracking without any beam-tracking external hardware. |
Table 1: MRI/US fusion devices commonly used in the United States and internationally. This table is adapted with permission from Elkhoury et al.17.
