Single slice SVI in a healthy subject
Specific ventilation imaging produces quantitative maps of specific ventilation as shown in Figure 3A, which depicts a single slice in the right lung of a 39-year-old healthy female. Note the presence of the expected vertical gradient in specific ventilation; the dependent portion of the lung presents higher specific ventilation than the non-dependent portion of the lung. A histogram of the mapped specific ventilation values is presented (Figure 3B, filled circles) along with a best-fit log-normal probability distribution function (dotted line). The width of the best-fit distribution can be used as a metric of specific ventilation heterogeneity7,23. Figure 1 shows a multiple breath washout acquired in the same subject, in the same posture. Figure 1A shows the temporal recording of nitrogen concentration measured at the mouth following a shift from inspired air to inspired 100% oxygen. Figure 1B presents the distribution of specific ventilation, as estimated from the washout. For both SVI and MBW, the relevant variable is the width of the distribution, as measured here by the width of a log normal distribution fitted to the data (dotted line), was found to be 0.41, using SVI and 0.42 using MBW within the healthy normal range. Validation of SVI-estimated specific ventilation heterogeneity by comparison with MBW was performed in 10 subjects and the difference between techniques was found to be smaller than the MBW inter-test variability7. A spatial comparison with a hyperpolarized gas multiple breath specific ventilation imaging16 also showed reliable group estimates of specific ventilation heterogeneity (the width of the specific ventilation distribution over the 8 subjects studied were 0.28 ± 0.08 and 0.27 ± 0.10 for hyperpolarized 3He and specific ventilation imaging, respectively), despite higher than expected intra-subject variability (the standard deviation of the individual differences in width was 0.13)16.
Specific ventilation maps can also be used in conjunction with lung density maps to compute regional alveolar ventilation. To generate maps of alveolar ventilation, specific ventilation and density images must be spatially smoothed to minimize the potential minor misalignments between the two modalities.
Response to methacholine challenge in an asthmatic subject
SVI can be used to measure both lung-wide and regional responses to interventions such as exercise4, posture2, or medication3. As an example, Figure 4 depicts single-slice maps from the lung of a mild asthmatic female subject at baseline (Figure 4A), following bronchoconstriction with methacholine (Figure 4B), and after albuterol-assisted recovery (Figure 4C). Note the increased specific ventilation heterogeneity during the induced asthma event, and the presence of large patches of little to no specific ventilation (dark blue regions in the dependent portion of the lung). Also, note that ventilation increased paradoxically in some regions during bronchoconstriction (green-red regions).
Multi-slice SVI
Up to six (typically four), contiguous, 15 mm lung slices can be simultaneously imaged with SVI. Figure 5 depicts four contiguous right lung slices, covering ~70% of the right lung, in a moderate asthmatic male subject who had been withdrawn from his asthma medications for 24 hours.
Ventilation map
Provided lung density information was acquired in the same slice, and the breathing frequency is known, a fully quantitative ventilation map can be computed in units of mL/min/mL. An example of a map of ventilation is shown in Figure 6.
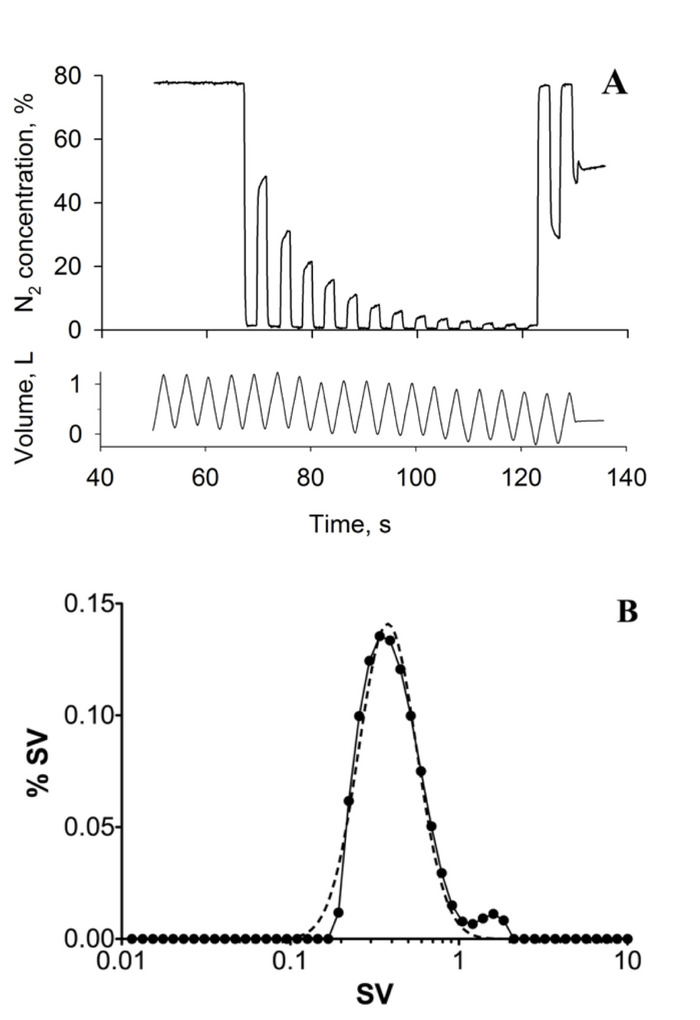
Figure 1: Multiple breath washout. (A) Typical MBW tracing showing expired nitrogen (N2) concentration (top) and tidal volume (bottom) over time (seconds, s). Data was acquired in the supine posture; the subject was a healthy 39-year-old female. (B) histogram depicting the distribution of specific ventilation (SV) computed from the MBW experiment using the method proposed by Lewis et al.23 (solid line). The dashed line represents the log(Gaussian) best fit to the specific ventilation distribution. The heterogeneity of specific ventilation, the key outcome, is measured as the width of the best fit distribution, in this case 0.42. This figure has been reprinted with permission from reference7. Please click here to view a larger version of this figure.
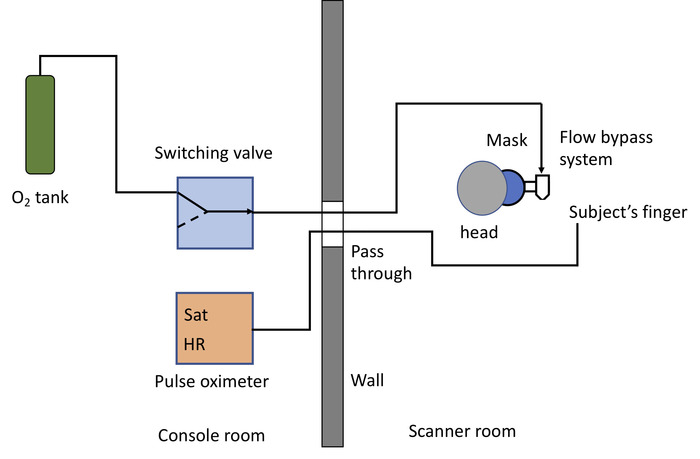
Figure 2: Diagram of the plumbing system and instrumentation. Specific ventilation imaging requires 100% medical oxygen, either from compressed gas tank (as drawn) or a wall outlet. The oxygen source is connected to a switch valve (control room), that in turn is connected, through the MRI pass-through, to the 3D printed flow bypass system24, attached to a facemask (scanner room). The left side of the drawing corresponds to the MRI control room, the right side to the scanner room. The plastic tubing connecting the tank to the switch is ¼ inch in diameter. The tubing from the switch valve outlet to the flow bypass system is also ¼ in. The last 2m include a step up in diameter, from ¼ inch to 3/8 inch, and then to ½ inch, in order to decrease the noise produced by the flow of air24. A pulse oximeter is used to monitor the subject’s heart rate (HR) and oxygen saturation (Sat) levels. Please click here to view a larger version of this figure.
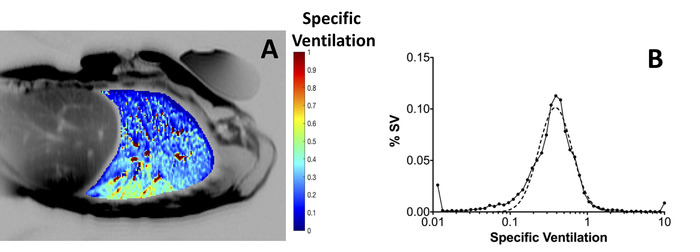
Figure 3: Specific ventilation imaging. (A) Typical map of specific ventilation (color), overlaid onto an anatomical MRI image of the same supine subject (gray scale). Specific ventilation ranges from very low values (blue) to SV = 1.0 (red). The subject, 39 year-old healthy volunteer (same subject as in Figure 1) was imaged in the supine posture. Note the vertical gradient in specific ventilation. A phantom of known MR characteristic used for calibration of absolute density was placed in the anterior chest wall. Phantoms are not required for SVI quantification. (B) Histogram of the distribution of specific ventilation (filled circles) compiled from the specific ventilation map. The width of the distribution represents the heterogeneity of specific ventilation in the lung slice studied. In this example, the distribution is unimodal and the width of the log Gaussian fitted distribution (dotted line) was 0.41; this is comparable to the MBW whole lung specific ventilation distribution presented in Figure 1B, for the same subject and posture, where the width of the distribution) was 0.42. Please click here to view a larger version of this figure.
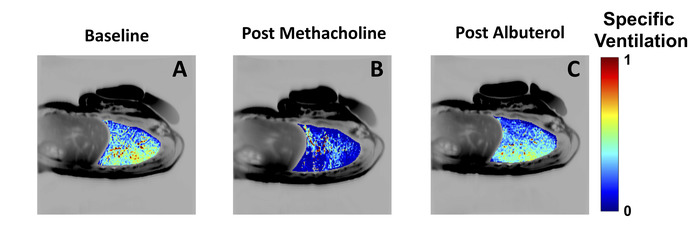
Figure 4: Bronchoconstriction and bronchodilation maps in a mild asthmatic. Specific ventilation measured in a mild asthmatic subject (female, age 24) at baseline (A), following inhalation of 1 mg/mL of methacholine (B) and following inhalation of albuterol (C). Note the significant changes in the distribution of specific ventilation following the induction of an asthma-like event using methacholine (panel B), with large regions of the dependent lung showing very low specific ventilation. Also note the recovery following bronchodilator administration (panel C). As in Figure 3, the specific ventilation maps have been overlaid into an anatomical MRI. The width of the specific ventilation distribution was 0.31 at baseline, 0.94 post methacholine, and 0.28 post albuterol. Please click here to view a larger version of this figure.
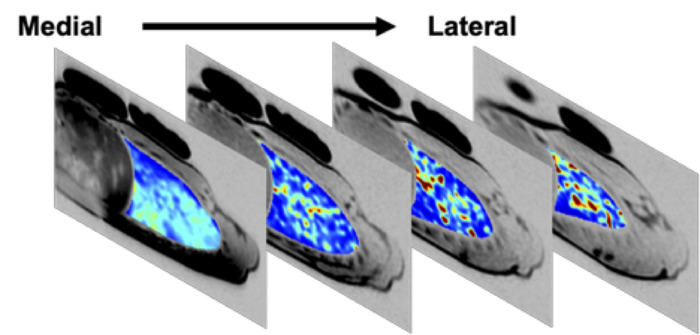
Figure 5: Multi slice specific ventilation map in a moderate asthmatic following 24-h medication withdrawal. Specific ventilation map of 4 contiguous lung slices in the right lung, acquired in a 25 year-old male moderate asthmatic after 24 h withdrawal of daily asthma medications. The 4 slices shown cover ~70% of the subject’s right lung. Regions of low specific ventilation (dark blue) are present in all slices. At baseline, FEV1 was 84% predicted. Following 24 h withdrawal of daily medications, this subject’s FEV1 was 69% of predicted; post-imaging, the subject used his rescue inhaler and FEV1 recovered to 83% of predicted. Please click here to view a larger version of this figure.
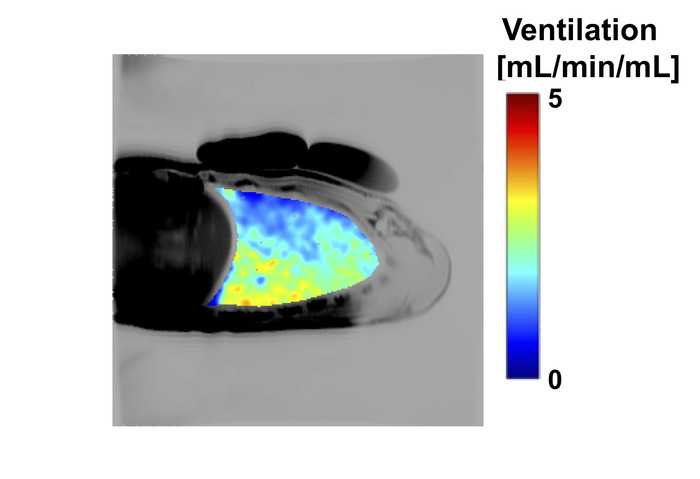
Figure 6: Example ventilation map showing ventilation (mL/min/mL) acquired in a healthy 27 year-old male subject. Ventilation maps were generated as described in section 6, using an SV map together with a map of lung proton density in the same slice. In this example, both the SV and density maps were smoothed using a log Gaussian kernel with a full width at half maximum of 5 voxels, resulting in a spatial scale of ~0.64 cm2 in plane. Please click here to view a larger version of this figure.
| MRI parameters | SVI | Notes |
| Echo time (TE) | 21.6 ms (single slice) | |
| 18.2 ms (multi slice) | ||
| Repetition time (TR) | 5 s | Any value > 4 s |
| Adjust for patient comfort | ||
| Inversion time (TI) | 1.100 s (single slice) | For multi slice, TI of slice n |
| 1.100, 1.335, 1.570, 1.805 s (4 slices) | TI(n)=1.100 s + 0.235*(n-1) | |
| Matrix | 256 x 128 (single slice) | |
| 128 x 128 (multi slice) | ||
| Field of View | 40 cm | 32-44 cm |
| Bandwidth | 125 kHz |
Table 1: List of typical MRI parameters used for acquisition of specific ventilation imaging.
