Fresh prostate tissue sampled using the PEOPLE method can be used for a variety of downstream techniques, including genomic sequencing and ex vivo culture. The first 59 cases sampled using this method have been previously published in comparison with an earlier version of the method, along with initial downstream data8. The time from first slicing the prostate to freezing/fixing the punch biopsies here was approximately 1 min, which was kept to a minimum to avoid degradation of RNA. Time from removal of the prostate to prostate slicing should also be kept to a minimum, though here this took approximately 20 min due to our theatre and pathology labs being in different locations.
Depending on the downstream application, typically at least two samples are taken: one from an area of anticipated tumor tissue and one from an area of anticipated benign tissue. The key measure of success for the sampling method itself is to assess the tumor content in a given sample.
For entry into the 100,000 genomes project, an H&E stained tissue section must be assessed by a uropathologist, and the sample must contain at least 40% tumor cells. Samples that contain less than 40% tumor may still be included in the project if they are successfully macrodissected. Of the first 92 cases sampled in this manner, 64% contained at least 40% tumor and were submitted to the 100,000 Genomes Project without macrodissection. DNA was extracted and was of sufficient yield and quality in all cases (Table 1). An initial subset of 59 of these samples was previously published in comparison with an earlier method8.
For ex vivo culture, matched tumor and benign tissue must be of sufficient quality to withstand 72 h culture without significant degradation. Multiple tissue samples from a total of three patients were cultured successfully8.
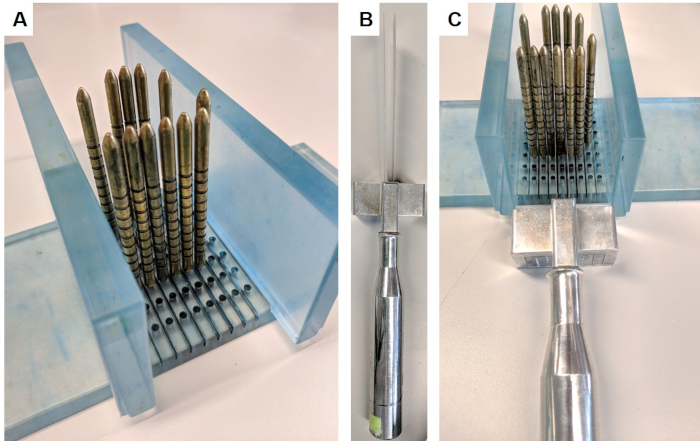
Figure 1: Prostate slicing apparatus. This apparatus was obtained under material transfer agreement from the Institute of Cancer Research. (A) The walls are inserted perpendicular to the base, and gold pins are inserted into the base surrounding the prostate (prostate not pictured). (B) The replaceable parallel blades are inserted into the blade handle. (C) The blades pass between the gold pins in order to slice a 5 mm section of the prostate. Please click here to view a larger version of this figure.
| n (%) | |
| Hit (>40% tumor) | 59 (64%) |
| Partial hit (5-30% tumor) | 6 (7%) |
| Miss (0% tumor) | 27 (29%) |
| Total | 92 (100%) |
Table 1: Tumor hit rate. Tumor hit rate was determined by a consultant pathologist specializing in prostate cancer, following review of H&E stained tissue. Tumor cell content of >40% was determined to be suitable for inclusion in the 100,000 Genomes Project, as per Genomics England guidelines.
