Observation at early ages: what and how to observe
Early childhood assessment in ordinary family contexts and at school is performed using the observational method. Hence, the evaluator must adhere to a precise observational process, the key to an accurate diagnosis and, therefore, to a successful training1. There are many development inventories that provide guidelines for assessment: The Portage Guide2, the Brunet Lézine Scale3, and the Battelle Developmental Inventory4, among others. These tools are based on internationally agreed standards set by the scientific community in the field of human evolutionary development. Although these tools analyze developmental areas (Psychomotor, Cognitive, Communication and Language, and Autonomy and Socialization), recent studies5 have proposed new tools that can also analyze these areas. These studies point out that the observational method from birth provides pointers of immense utility to early intervention and for the early detection of pathologies. However, the observational processes at these ages are complex, as they depend on behavioral observations recorded in natural contexts, which are not always easy to carry out.
Within this framework, the assessment of the acquisition of functional abilities at early ages is of great interest to parents, educators, and therapists alike. Any such assessment is of relevance for children who have been diagnosed or who are at risk of developing some disability. Early detection of developmental disorders is essential for the early diagnosis and intervention. Observational study from birth will provide indicators of this early detection and intervention5. Currently there are various tools (development inventories, scales, tests, etc.) for measuring development at those ages. The instruments that can currently be applied are developmental inventories, some of which are standardized. However, some of those instruments may require knowledge of psychometric techniques and the results are not automatically displayed on screen. For this reason, it is important to develop other tools that are easier to use and interpret.
Preparation of software for recording and interpreting data from the processes of contextual observation processes at early ages
The software development was, therefore, considered of relevance, which would assist the observers (therapist, educator, etc.) to record and to interpret the results of their observations. This protocol and software, eEarlyCare, can be used both in educational centers that work with children with disabilities and in therapeutic intervention centers aimed at this group. This is why from now on the term "user "will be used, which includes both students and patients, depending on the place where the intervention is carried out. In particular, a software that could facilitate the recording and the interpretation of data gathered in natural contexts from the observation of functional abilities among children from 0 to 6 years old. This software, eEarlyCare, is based on the functional abilities scale6 [Scale for the measurement of Functional Abilities in children between 0-6 years old] (SFA); this scale includes the measurement of 11 areas of development (Food Autonomy, Personal Care and Hygiene, Independently and dress and undresses, Sphincter control, Functional mobility, Communication and Language, Interactive symbolic play, Daily life routines, Adaptive behavior). Also, it was in turn, inspired by the Portage Guide2, the Pediatric Evaluation of Disability Inventory (PEDI)7, and the works of Bronson8, as well as Whitebread and Basilio4 on social skills at ages 0-6, the Brunet-Lézine Scale3, developmental inventories for children aged 0-67, and the Assessment Scale of the precursors9 to social skills. This tool is a computer application that is used for registering the results of each user assessment in longitudinal follow-ups (quarterly, monthly, annual, etc.). It is a referential aspect for the therapist with regard to the intervention, and for other professionals who work with children in early childhood with suspected dysfunctionalities. In addition, the software10 can automatically produce comparisons between the development of the functional abilities of different users, regardless of whether they are at the same intervention center, thereby facilitating the definition of common aspects for collaborative work.
In particular, this software is based on mainstream technologies (e.g., Windows Presentation Foundation Development -WPF-11), a technological innovation that integrates advanced graphics to produce accurate graphic results12 and a positive computer user-experience. The quality of the graphs improves the visualizations and the interactivity available with other tools such as spreadsheets. The application can store the data locally on relational databases and upload the information onto the cloud to be shared. In addition, the classic client-server architecture is also supported. These features make it easy to record the data that are collected from the observations and to process the results for visualization. Also, once registered, it is very easy to export the data. This allows the data to be used in powerful statistical packages to apply data mining techniques, such as supervised (classification and/or regression) and unsupervised (grouping) machine learning.
In this study, the classification techniques are of specific utility for personalized learning13. The architecture can be seen in Figure 1 and Figure 2. In Figure 1, the functionality of cloud storage is used as a safeguard, in case of data security problems and potential loss and corruption of data when exchanged between applications. Additionally, the software can also operate in a classic network-based client-server architecture with a database (Figure 2) with all data exchanges taking place between clients (these are concepts that are used in the field of computer science). These platforms provide authentication mechanisms and restricted access, which ensure privacy and data protection, while facilitating interaction with fully developed applications. The final result is an application interface that is designed14 for early-care professionals, so that they can use Learning Analytics techniques in a simple way and refer to them, in order to follow up the degree of each student’s development in each evaluation area of the scale15.
The application also offers a general profile of each user in each of the functional areas and subareas (Table 1). It also produces a comparison between all users at any one center. In brief, it produces a personalized analysis of the intervention needs of the different users. In addition, it helps early-care professionals with their intervention programs, as it can flag up areas in which users might or might not show similar developmental patterns. All these results guide the type of intervention programs that can be used together, rather than those that have to be designed individually. The data that are linked to this interface are the SFA scores of the users that are measured on a Likert scale from 1 to 5. Those scores can be compared with the maximum developmental age scores linked to each SFA dimension. The software can also link the chronological age of each user to the developmental age of each SFA dimension; a relevant aspect for the detection of intervention areas from among which to prioritize the areas for treatment.
| Functional area | Functional sub-area |
| 1. Food Autonomy | 1. Food Texture |
| 2. Use of utensils | |
| 2. Personal Care and Hygiene | 3. Dental Hygiene |
| 4. Hairstyle | |
| 5. Nasal Care | |
| 6. Handwashing | |
| 7. Face and body wash | |
| 3. Independently dresses and undresses | 8. Dressing and undressing (waist upwards) |
| Dressing and undressing (waist downwards) | |
| 4. Sphincter control | 9. Sphincter control |
| 5. Functional mobility | 10. Upper extremity |
| 11. Transfers in WC | |
| 12. Transfers on a chair | |
| 13. Mobility and bed transfers | |
| 14. Mobility in the bathtub | |
| 15. Mobility indoors | |
| 16. Transport of objects | |
| 17. Outdoor Mobility | |
| 6. Communication and Language | 18. Word comprehension |
| 19. Understanding phrases | |
| 20. Functional use of communication | |
| 7. Resolution of tasks in social contexts | 21. Solving Problems |
| 22. Information about yourself | |
| 8. Interactive and symbolic play | 23. Interactive Play |
| 24. Interaction with the peer group | |
| 25. Play with objects | |
| 9. Daily life routines | 26. Guidance in time |
| 27. Homework | |
| 10. Adaptive behavior | 28. Self-harm behavior |
| 29. heteroagressiveness (harming others) | |
| 30. Destruction of objects | |
| 31. Disruptive behaviour (cry, shout, laugh without reason) | |
| 32. Stereotypes | |
| 11. Attention | 33. Attention |
Table 1: List of functional areas and subareas.
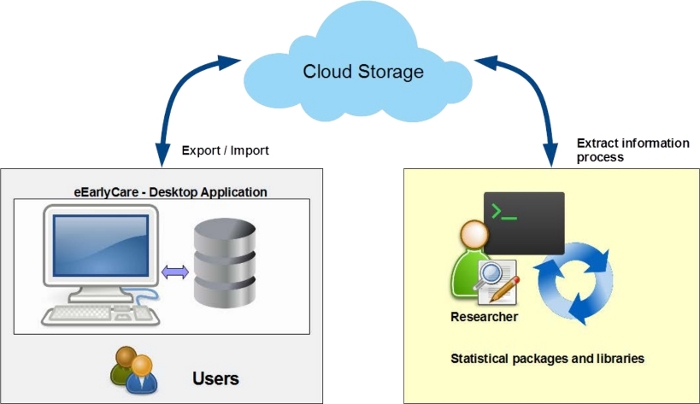
Figure 1: Architecture of the proposal of automation of the correction of the Scale functionality of cloud storage. Please click here to view a larger version of this figure.
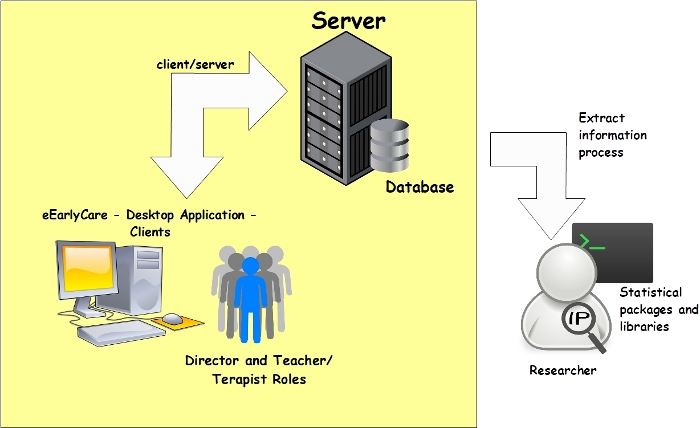
Figure 2: Architecture of the proposal of automation of the correction of the Scale functionality classic network. Please click here to view a larger version of this figure.
Therapists and intervention professionals can use this assessment protocol and the software implementation for the assessment of functional abilities and their development in early childhood between 0 and 6 years of development. The software can be used with children within that age range, although it is especially useful for children with suspected impaired development of functional abilities. It is likewise especially useful at Special Education Centers. The Research question is whether, having observed the functional abilities of children, the use of a computer tool will facilitate the recording and the interpretation of the results for the therapist.
The present study recruited 11 participants with confirmed diagnoses [both moderate (development quotient = DQ 40-65) and severe (DQ 39-60) intellectual disabilities]. The protocol was tested in a pilot project over 20 months at a Special Education Center. All the diagnoses for this study had been confirmed by a multidisciplinary team in accordance with DSM-5, using the Brunet Lézine Scale, as the degree of affectation was beyond the scope of other scales such as the Wechsler Preschool and Primary Scale of Intelligence (WPPSI). However, the ages of the participants slightly exceeded the chronological age of 6 (Table 2). The actions carried out and the application times in this study can be found in Table 3.
| Functional area | Time | Location | Responsible* |
| Food Autonomy | 1 week | During meals in natural contexts. | Teacher or Therapist |
| Personal Care and Hygiene | 1 week | In care and hygiene activities in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Dressing and undressing independently | 1 week | During the task of dressing and undressing in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Control of sphincters | 1 week | During the daytime in the natural context. | Teacher or Therapist |
| (center or home) | |||
| Functional mobility | 1 week | During the activities of daily life in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Communication and language | 1 week | During the activities of daily life in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Resolution of tasks in social contexts | 1 week | During activities of daily living in natural contexts | Teacher or Therapist |
| (center or home) | |||
| Interactive and symbolic play | 1 week | Situations of symbolic play in natural contexts., | Teacher or Therapist |
| (center or home) | |||
| Daily life routines | 1 week | During the activities of daily life in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Adaptive behavior | 1 week | During the activities of daily life in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| Attention | 1 week | During the activities of daily life in natural contexts. | Teacher or Therapist |
| (center or home) | |||
| NOTE: *Either the teacher or the therapist will contrast the results of the observations gathered at the center with the information gathered from the family, to see whether there are any discrepancies. Prior agreement and consent were always sought from the family, before observation at home in natural contexts that were recorded in video format for subsequent analysis. The number of observations was established according to the type of functional ability, establishing the criterion of different observations during one week in a natural context (center or home). | |||
Table 3: Process to observation in different functional areas.
A comparative analysis can be performed once the professional (teacher or therapist) enters the data in the software. The development of users (students or patients) from the same classroom on the different dimensions of the scale is shown.
In this study, we present some examples of data analysis with the observational protocol coupled with the use of the software. We first performed a cluster analysis, in order to check whether the diagnoses of both medium and severe intellectual disabilities of the children with special educational needs corresponded to their actual development. Using the k-means method, we found 2 clusters belonging to either group. Cluster 1 and Cluster 2 integrated 55% and 45% of the sample, respectively. A cross-table was then constructed to study the relationship between membership of a group cluster and the variable ‘degree of disability’. It was found that all the subjects grouped in Cluster 1 belonged to group a) (moderate intellectual disabilities) and Cluster 2 included all the students belonging to group b) (severe intellectual disabilities) and there was only one with moderate intellectual disabilities (Table 4). A Cohen Kappa coefficient = .820, p = .006 was obtained.
| Cluster case number | Total | |||
| 1 | 2 | |||
| Disabilities | a | 5 | 0 | 5 |
| b | 1 | 5 | 6 | |
| Total | 6 | 5 | 11 | |
Table 4: Cross Table Disability Cluster Case Number.
The software can, therefore, record the development of the functional abilities of the children under treatment at the same (education or therapy) center and can determine similar and different levels of development. This aspect is very important, as it will facilitate the application of similar intervention programs among children with similar needs, which will in turn facilitate personalized intervention and efficient use of resources.
Progressing with this analysis, a study can be performed of the abilities of the participants in each functional group (disability moderate vs. disability severe). Both Spider and specific bar graphs were used for this purpose see Figure 3 and Figure 4.
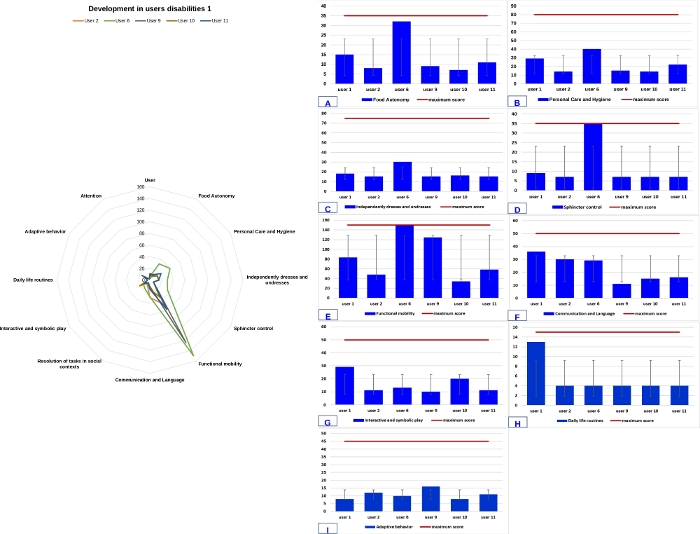
Figure 3: Comparative analysis between development of each user (student or patient) and the expected development in children with several intellectual disabilities.
(A) Food Autonomy, (B) Personal Care and Hygiene, (C) Independently dress and undresses, (D) Sphincter control, (E) Functional mobility, (F) Communication and Language, (G) Interactive and symbolic play, (H) Daily life routines, (I) Adaptive behavior. Blue line indicates skill acquisition score. Garnet line indicates maximum score. Error bars included in A, B, C, D, E, F, G, H and I. The error bars are graphical representations of data variability, an error bar indicates the uncertainty of a value. The x-axis represents the participants (with several intellectual disabilities) and the y-axis represents the scores they have obtained in each functional area. The spider graph shows the comparative development of the participants in each functional area. Please click here to view a larger version of this figure.
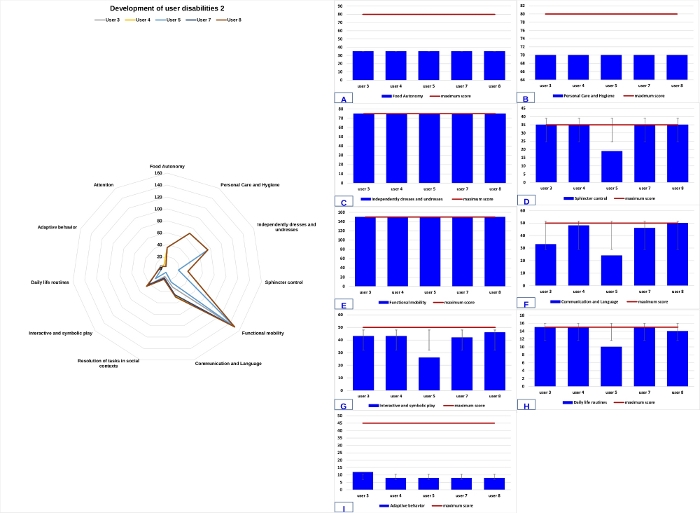
Figure 4: Comparative analysis between development of each user (student or patient) and the expected development in children with moderate disabilities.
(A) Food Autonomy, (B) Personal Care and Hygiene, (C) Independently dress and undresses, (D) Sphincter control, (E) Functional mobility, (F) Communication and Language, (G) Interactive and symbolic play, (H) Daily life routines, (I) Adaptive behavior. Blue line indicates skill acquisition score. Garnet line indicates maximum score. Error bars included in A, B, C, D, E, F, G, H and I. The error bars are graphical representations of data variability, an error bar indicates the uncertainty of a value. The x-axis represents the participants (with moderate intellectual disabilities) and the y-axis represents the scores they have obtained in each functional area. The spider graph shows the comparative development of the participants in each functional area. Please click here to view a larger version of this figure.
