These results in ECPs and LCPs have previously been published by Facer-Childs, Campos, et al.23. All permissions have been obtained from the publisher. For studies requiring an investigation of all three groups (Early, Intermediate and Late), the same methods and cut offs can be used.
Circadian Phenotyping (Table 1, Table 2 and Figure 1)
The first hypothesis presented in this paper is that the groups would differ significantly in sleep and circadian variables. From the participants (n = 22) that took part in this study, those that were categorized as ECPs had a score between 0-1 and all LCPs between 8-10 (cuts off given in Table 1). To confirm these results, group averages were compared for each variable. MSFsc was 02:24 ± 00:10 h for ECPs compared to 06:52 ± 00:17 h in LCPs (t(36) = 12.2, p < 0.0001). Physiological markers also differed significantly between the two groups. DLMO occurred at 20:27 ± 00:16 h in ECPs and at 23:55 ± 00:26 h in LCPS (t(30) = 6.8, p < 0.0001). Peak time of the cortisol awakening response occurred at 07:04 ± 00:16 h in ECPs and 11:13 ± 00:23 h in LCPs (t(36) = 8.0, p < 0.0001). The same relationships were observed with actigraphic variables for sleep onset and wake up timings with average sleep onset occurring at 22:57 ± 00:10 h in ECPs and 02:27 ± 00:19 h in LCPs (t(34) = 8.9, p < 0.0001) and wake up time occurring at 06:33 ± 0.10 h in ECPs and 10:13 ± 00:18 h in LCPs (t(34) = 9.9, p < 0.0001). Other sleep variables including duration, efficiency and latency did not differ significantly between the groups (Table 2).
The second hypothesis is that MSFsc gathered from the MCTQ would be significantly correlated with the gold standard actigraphic and circadian phase biomarkers. Figure 1 shows that MSFsc was significantly correlated with DLMO (R2 = 0.65, p < 0.0001), peak time of cortisol awakening response (R2 = 0.75, p < 0.0001), sleep onset (R2 = 0.80, p < 0.0001) and wake up time (R2 = 0.86, p < 0.0001).
These representative results show that the different circadian phenotype groups have clear differences in sleep onset/offset (i.e., wake up time), as well as in physiological variables (DLMO and peak time of morning cortisol).
Diurnal Testing (Figure 2)
It was hypothesized that by testing multiple times over the course of the day, diurnal rhythms in subjective sleepiness and performance would be able to be identified in each group (ECPs/LCPs). In addition, it was hypothesized that if circadian phenotypes were not considered and data were analyzed at a whole group level only, then diurnal variations would be misrepresented.
Significant diurnal variations were found at the whole group level for the PVT and KSS. PVT performance at the 08:00 h testing session was significantly slower than the 14:00 h test (p = 0.027), as was subjective sleepiness (p = 0.024). Significantly slower PVT performance was also found between 08:00 h and 20:00 h (p = 0.041).
When each group was analyzed separately, significant diurnal variations in PVT performance were found in LCPs but not in ECPs. LCPs were significantly worse at 08:00 h compared to 14:00 h (p = 0.0079) and better at 20:00 h compared to 08:00 h (p = 0.0006). Subjective sleepiness showed significant diurnal variations within each group. ECPs reported higher sleepiness at 20:00 h compared to 08:00 h (p = 0.0054). The opposite was observed in LCPs who reported highest sleepiness at 08:00 h and lowest at 20:00 h. Sleepiness at 08:00 h was significantly higher than 14:00 h and 20:00 h in LCPs (both p < 0.0001).
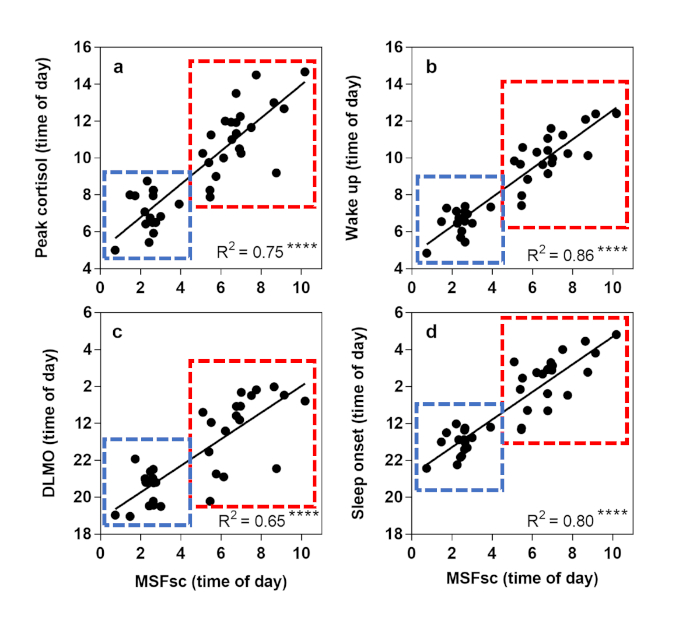
Figure 1: Linear regression analysis to show relationships between sleep/wake variables using actigraphy and physiological biomarkers. Corrected mid-sleep on free days (MSFsc) is displayed as time of day (h) on the x axis. Early circadian phenotypes (ECPs) are shown in the blue box, Late circadian phenotypes (LCPs) in the red box. (a) Peak time of cortisol awakening response (h), (b) Wake up time (h), (c) Dim light melatonin onset (DLMO) (h), (d) Sleep onset time (h). R2 value is shown in the bottom right corner with significance level displayed at **** = p < 0.0001. This figure has been modified, with permission, from Facer-Childs, et al.23. Please click here to view a larger version of this figure.
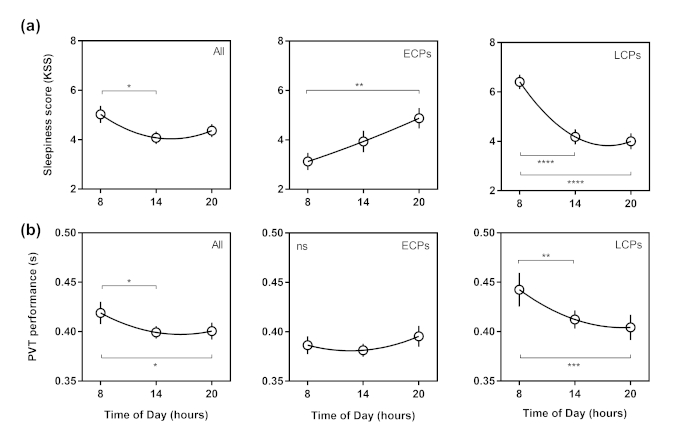
Figure 2: Diurnal variations curves in Karolinska Sleepiness Scale and Psychomotor Vigilance Task (PVT) performance. Time of day (h) is shown on the x axis. Whole group results are shown in the first column, Early circadian phenotypes (ECPs) in the second column and Late circadian phenotypes (LCPs) in the third column. (a) Subjective sleepiness (KSS) score, (b) Reaction time from PVT (s). Second order polynomial non-linear regression curves have been fitted. Significance level is shown as ns (not significant), * (p < 0.05), ** (p < 0.01), *** (p < 0.001) and **** (p < 0.0001). This figure has been modified, with permission, from Facer-Childs, et al.23. Please click here to view a larger version of this figure.
| Variable measured | ECP Category | ICP Category | LCP Category |
| Actigraphic wake up time | < 07:30 h | 07:31 – 08:29 h | > 08:30 h |
| Peak time of morning cortisol | < 08:00 | 08:01 – 08:59 h | > 09:00 h |
| Dim light melatonin onset (DLMO) | < 21:30 h | 21:31 – 22:29 h | > 22.30 h |
| Actigraphic sleep onset | < 23:30 h | 23:31 – 00:29 h | > 00:30 h |
| Corrected mid-sleep on free days (MSFsc) | < 04:00 h | 04:01 – 04:59 h | > 05:00 h |
| Score per variable | 0 | 1 | 2 |
| TOTAL SCORE | 0 – 3 | 4 – 6 | 7 – 10 |
| Subcategories | 0 = extreme ECP 1 = definite ECP 2 = moderate ECP 3 = mild ECP |
4 = early ICP 5 = ICP 6 = late ICP |
7 = mild LCP 8 = moderate LCP 9 = definite LCP 10 = extreme LCP |
Table 1: Categorization cut offs for circadian phenotyping into Early (ECP), Intermediate (ICP) and Late (LCP) groups. Each variable is allocated a score per participant depending on their result and total scores (0-10) allow categorization into each group and each sub-category.
| Variable Measured | ECPs | LCPs | Significance |
| Sample Size | N = 16 | N = 22 | n/a |
| Number of Males/Females | M = 7 | M = 7 | p = 0.51c |
| F = 9 | F = 15 | ||
| Age (years) | 24.69 ± 4.60 | 21.32 ± 3.27 years | p = 0.028a |
| Height (cm) | 171.30 ± 1.97 | 171.10 ± 2.38 | p = 0.97a |
| Weight (kg) | 66.44 ± 2.78 | 67.05 ± 2.10 | p = 0.88a |
| MSFsc (hh:mm) | 02:24 ± 00:10 | 06:52 ± 00:17 | p < 0.0001a |
| Sleep Onset (hh:mm) | 22:57 ± 00:10 | 02:27 ± 00:19 | p < 0.0001a |
| Wake Up Time (hh:mm) | 06:33 ± 0.10 | 10:13 ± 00:18 | p < 0.0001a |
| Sleep Duration (h) | 7.59 ± 0.18 | 7.70 ± 0.14 | p = 0.72a |
| Sleep Efficiency (%) | 79.29 ± 1.96 | 77.23 ± 1.14 | p = 0.46a |
| Sleep Onset Latency (hh:mm) | 00:25 ± 00:06 | 00:25 ± 00:03 | p = 0.30b |
| Phase Angle (hh:mm) | 02:28 ± 00:16 | 02:34 ± 00:18 | p = 0.84a |
| Dim Light Melatonin Onset (hh:mm) | 20:27 ± 00:16 | 23:55 ± 00:26 | p < 0.0001a |
| Cortisol Peak Time (hh:mm) | 07:04 ± 00:16 | 11:13 ± 00:23 | p < 0.0001a |
Table 2: Study variables for circadian phenotype groups; Early (ECPs) and Late (LCPs). Values are shown as mean ± SEM apart from age which is shown as mean ± SD. Corrected mid-sleep on free days (MSFsc) is calculated from the MCTQ. Type of statistical tests used are shown in superscript; parametric testsa, non-parametric testsb and Fisher's exact testc. Phase angle is determined by the difference (h) between dim light melatonin onset (DLMO) and sleep onset. All p values are FDR corrected24. This Table has been modified, with permission, from Facer-Childs, et al.23.
