The ANGIO Mentor simulator was previously shown to improve the skills of surgical trainees with varying neuroendovascular experience when performing simulated diagnostic angiograms, thrombectomies, and ruptured aneurysm coil embolizations in an academic setting2. In this study, performance metrics for the aforementioned procedures were established over the course of 30 days in one medical student, one neurosurgery resident, two diagnostic neuroradiology fellows, and one endovascular neurosurgery fellow. After 120 minutes of didactic instruction and a single viewing of each procedure, the trainees performed 10 sessions of each procedure (i.e., 30 total). Procedural evaluations were performed by an experienced neurointerventional attending based on total procedural time, fluoroscopy time, contrast dose, frequency of technically unsafe events (e.g., movements with insufficient leading wire, rapid forward/non-visualized device movements, accidental vessel catheterizations, coil deployments outside of the aneurysm, and number of intraprocedural ruptures), packing densities, number of coils used, and number of stent retriever passes attempted.
Based on analysis of variance (ANOVA) and Tukey’s Honest Significant Difference (HSD) testing, statistically significant improvements were seen among all participants in specific performance metrics for all three procedures, including contrast utilization, fluoroscopy time, and total procedural time (Figure 2), in addition to significantly increased Likert Scale scores, an evaluation gauge in which a score of 1 corresponds to failure and 5 corresponds to excellence based on procedural technique (Figure 3). Notably, training on diagnostic angiograms resulted in an 86% reduction in total procedure time, a 75% reduction in fluoroscopy time, a 68% reduction in contrast utilization, and a 64% improvement in the overall Likert Scale performance scale (p < 0.05 for all variables based on performance improvements in the first five angiograms). After mechanical thrombectomy simulation, trainees demonstrated a 35% reduction in total procedure time, a 41% reduction in fluoroscopy time, a 49% reduction in contrast utilization, and a 67% improvement in overall Likert Scale performance (p < 0.05 for all variables based on performance improvements in the first five procedures). Participants also showed statistically significant improvements in performance after simulated aneurysm coilings, with a 42% reduction in total procedure time, a 57% reduction in fluoroscopy time, a 21% reduction in contrast utilization, and a 58% improvement in Likert Scale score (p < 0.05 for all variables based on performance improvements in the first five procedures). A reduction in the occurrence of unsafe events was also seen across all scenarios. Based on these data, at our institution all neuroendovascular trainees perform five simulated angiograms, five simulated thrombectomies, and ten simulated aneurysm permanent coil embolizations (the higher number or embolizations based on the technical nuances of this procedure), prior to participating in a surgery with real neuroendovascular cases.
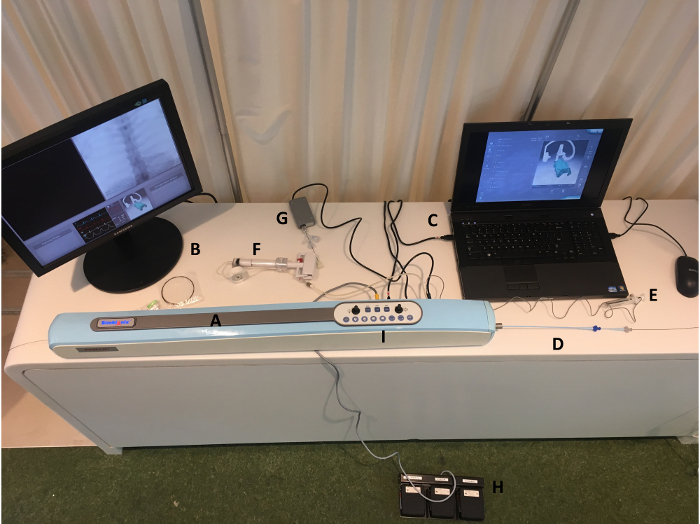
Figure 1: ANGIO Mentor Simulator complete assembly. The setup for the ANGIO Mentor simulator includes the simulator housing (A); an external monitor for image projection (X-ray, angiography) (B); a laptop for interfacing with the Simbionix Software (C); the simulated femoral artery sheath with an outer guide catheter, inner diagnostic microcatheter, and guidewire shown (D); a contrast syringe (E); an insufflator for balloon inflation not used in these patient scenarios (F); a stent delivery device not used in these patient scenarios (G); foot pedals for fluoroscopy, roadmap guidance, and angiographic runs (H); and the operator control panel on the simulator housing where the operator is able to control patient and image intensifier positioning (I). The image was obtained by the authors after setting up the simulator. Please click here to view a larger version of this figure.
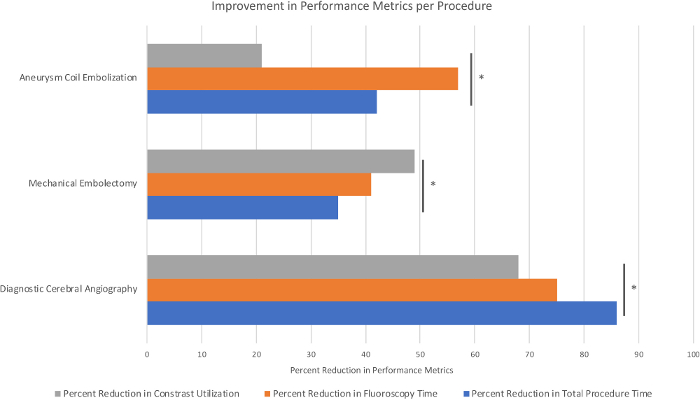
Figure 2: Performance evaluation represented as percent reduction in associated measured procedure metrics with simulator training. Sample size, n = 5 trainees, performing 10 simulations per procedure (Pannell, et al.)2. *p < 0.05 based on analysis of variance (ANOVA) and Tukey’s Honest Significant Difference (HSD) testing. Please click here to view a larger version of this figure.
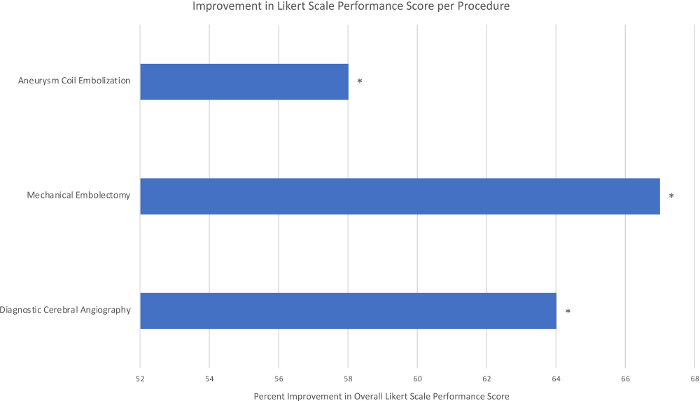
Figure 3: Performance evaluation represented as percent improvement in overall Likert Scale Score with simulator training. Sample size, n = 5 trainees, performing 10 simulations per procedure (Pannell, et al.).2 *p < 0.05 based on analysis of variance (ANOVA) and Tukey’s Honest Significant Difference (HSD) testing. Please click here to view a larger version of this figure.
| Patient Scenario #1 |
| 1) 5-French femoral sheath |
| 2) 0.035 inch guidewire |
| 3) 4-French diagnostic catheter |
| Patient Scenario #2 |
| 1) 0.035 inch guidewire |
| 2) 4-French diagnostic catheter |
| 3) 6-French guide catheter |
| 4) Microcatheter/microwire |
| 5) Coils |
| Patient Scenario #3 |
| 2) 0.035 inch guidewire |
| 3) 4-French diagnostic catheter |
| 4) 6-French guide catheter |
| 6) Microcatheter/microwire |
| 7) Stent retriever device |
Table 1: Materials used for each scenario.
