DMM-induced OA results in articular cartilage degeneration and chondrocyte loss
DMM-induced OA resulted in an increased OARSI score compared to sham mice, distinctly characterized by surface erosion and cartilage loss (Figure 1A,D). The histomorphometry protocol detailed here detected several OA-associated changes, including a decrease in total cartilage area and in the uncalcified cartilage area (Figure 1A,B,E,G); reduction in the total chondrocyte number; and, importantly, loss of matrix producing chondrocytes (Figure 1H,I). Changes to the articular surface, indicative of the severity of erosion, were evaluated using the cartilage fibrillation index. Overall, the fibrillation index increased in DMM mice (Figure 1C,K,L). However, it is also important to note that the fibrillation index may decrease in end-stage OA due to complete erosion of the cartilage surface, as discussed in the Protocol. An increase in the fibrillation index signifies degeneration of the articular cartilage surface during OA development and progression. These results highlight the ability of the histomorphometric analysis program to detect and quantify pathological cartilage changes that characterize OA progression.
Assessment of other joint changes in DMM-induced OA
OA affects joint tissues other than the cartilage, and pathological changes in these tissues play a crucial role in disease progression. Here, the described histomorphometric analysis method revealed an increase in the subchondral bone area and a reduction in the area of the bone marrow space in DMM mice (Figure 2A–D), indicating subchondral bone sclerosis29,30. Both anterior and posterior osteophyte areas also increased in DMM mice (Figure 2E,F), suggesting an ongoing subchondral bone remodeling that acts as a compensatory mechanism to handle changes in joint loading at the site of injury29,30.
Histomorphometric analysis of the synovium showed increased synovial thickness in DMM mice (Figure 3A–C), which is a typical outcome of OA-associated synovial inflammation and the diffusion of inflammatory cytokines into the joint space11,12,31,32,33,34.
Analysis of interuser variability between OARSI scoring versus histomorphometry
Figure 4A shows no significant interuser variability of both histomorphometric analysis of the uncalcified cartilage area (Figure 4A) and the OARSI score (Figure 4B). However, the histomorphometric analysis showed an extremely low mean difference in between observers ranging from -0.0001179–0.00120, leading to an almost complete overlap of the results obtained by the three observers, while the mean difference between observers was higher in the OARSI score ranging from -0.3–0.3 with a clear deviation of O1 values from O2 and O3 values.
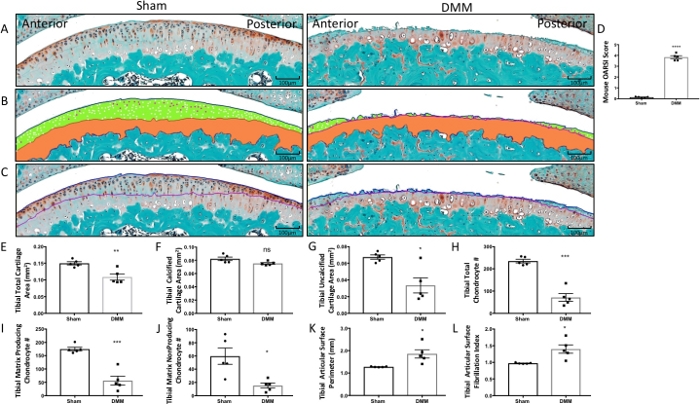
Figure 1: Histomorphometry of tibial articular cartilage and articular chondrocyte phenotypes from sham surgery and DMM mice. (A) Tibial articular surface stained with Safranin-O/Fast Green. (B) Histomorphometric analysis was used to trace the total cartilage area and the calcified cartilage area (orange). The cartilage superior to the tidemark area was calculated as the uncalcified cartilage (green). Matrix producing chondrocytes (white) and matrix nonproducing chondrocytes (magenta) were counted within the uncalcified cartilage area. (C) The tibial articular surface perimeter was measured by tracing the articular surface (blue line) followed by the tidemark (purple line) to determine the fibrillation index. (D) The OARSI score increased in DMM mice. (E–L) Graphical representation of the quantified cartilage areas and chondrocyte counts from sham and DMM mice. Compared to sham mice, DMM mice had decreased total tibial cartilage area (E), tibial calcified cartilage area (F), tibial uncalcified cartilage (G), tibial total chondrocyte number (H), tibial matrix producing chondrocytes, (I) and tibial matrix nonproducing chondrocytes (J). Compared to sham mice, DMM mice had increased tibial articular surface perimeter (K) and increased tibial articular surface fibrillation index (L). Images were taken using 10x magnification. *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001 using unpaired t-test with Welch’s correction, values are expressed as mean ± SEM; n = 5/group. Please click here to view a larger version of this figure.
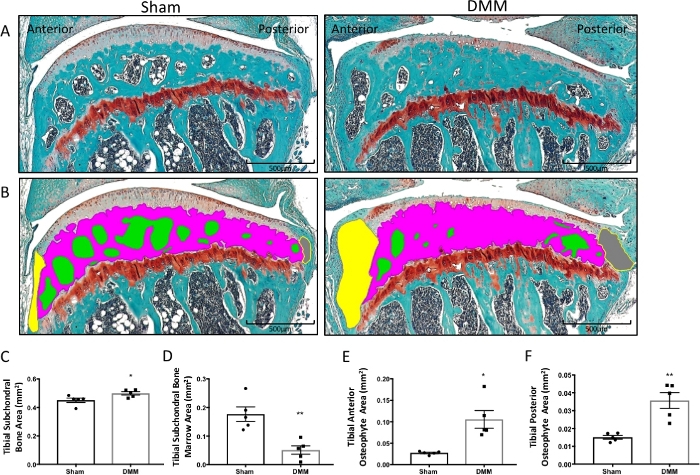
Figure 2: Histomorphometry of subchondral bone marrow area and subchondral bone area from sham surgery and DMM mice. (A) Tibial articular cartilage and subchondral bone stained with Safranin-O/Fast Green. (B) The subchondral bone marrow areas (green), subchondral bone area (magenta), anterior osteophyte area (yellow), and posterior osteophyte area (gray) were traced with computed histomorphometry software. (C–F) Graphed histomorphometric areas between the sham and DMM mice. Compared to the sham mice, DMM mice had an increased tibial subchondral bone area (C) and tibial anterior and posterior osteophyte areas (E–F), as well as decreased tibial subchondral bone marrow area compared to sham mice (D). Images were taken using 4x magnification. *P < 0.05, **P < 0.01 using unpaired t-test with Welch’s correction. Values are expressed as mean ± SEM; n = 5/group. Please click here to view a larger version of this figure.
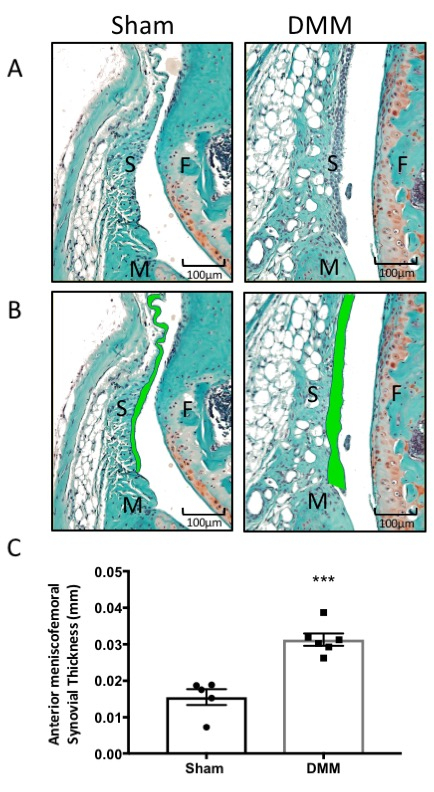
Figure 3: Histomorphometry of synovium from sham surgery and DMM mice. (A) Synovium stained with Safranin-O/Fast Green. (B) The synovial thickness was measured by tracing the anterior meniscofemoral synovial membrane across the anterior aspect of the tibiofemoral joint (green). (C) Graphical representation of synovial thickness measurements using computed histomorphometry software. DMM mice had an increased synovial thickness compared to sham mice. Images were taken at 20x magnification. ***P < 0.001 using unpaired t-test with Welch’s correction, values are expressed as mean ± SEM; n = 5/group; S = synovium; F = femur; and M = meniscus. Please click here to view a larger version of this figure.
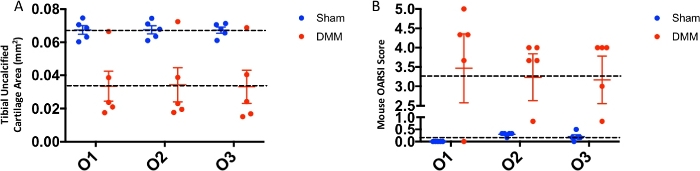
Figure 4: Interuser variability in OARSI scoring versus histomorphometric analysis. (A) Uncalcified cartilage area measurements obtained using histomorphometry by three blinded observers (O1, O2, O3). (B) OARSI scores for sham and DMM mice obtained from the three blinded observers. The dotted lines denote the mean value for each group. Please click here to view a larger version of this figure.
Supplementary Figure 1: Histological analysis of Safranin-O and Fast Green stained mouse tibiofemoral joint sections. (A) A 4x magnification image of the tibiofemoral joint. Areas of focus are labeled. (B) A 10x magnification image of the tibiofemoral joint ROI. The tibial and femoral surfaces as well as the anterior and posterior meniscal horns are visualized. The menisci are approximately the same size and the imaging ROI is centered on the joint compartment. (C) A 40x magnification image of the proximal tibial surface. The tidemark line is labeled as the line between the uncalcified and calcified cartilage zones. The osteochondral junction is labeled between the end of the calcified cartilage and beginning of the subchondral bone. Please click here to download this figure.
Supplementary Figure 2: Histomorphometry system setup and camera white balance calibration. (A) Mouse tibiofemoral joint visualized at 4x magnification in the software window with white balance not set. Note the camera settings tab at the top of the screen and the selection in the dropdown menu to set the white balance. (B) Mouse tibiofemoral joint at 4x magnification with white balance set. Note the change in the coloration and staining of the sample, increasing the user’s ability to distinguish certain areas of the tibiofemoral joint when performing measurements. Please click here to download this figure.
Supplementary Figure 3: Setup of histomorphometric software prior to histomorphometric analysis measurements. Representative screenshot of the histomorphometric software window. Note the stained mouse knee section is centered in the measurement region (yellow grid) and the correct magnification scale for the region is selected to match the objective being used on the microscope (circled in red in the top right hand corner of the screen). The list of parameters is displayed in the column to the right of the imaging and measurement area. Selecting a parameter will highlight the parameter, hence Tibial Fibrillation is currently selected to be measured. The Summary Data tab at the bottom of the window is where measurements for each parameter for each sample will be organized and saved to be exported following completion of each parameter measurement for each section. Please click here to download this figure.
