The following procedures were conducted according to the recommendations of the Declaration of Helsinki and Tokyo and the Guidelines for the Use of Experimental Animals of the European Community. The experiments were also approved by the Animal Care Committee at the Ben-Gurion University of the Negev.
1. Preparing rats for the experimental procedure
- Select adult male Sprague-Dawley rats without overt pathology, each weighing between 300 and 350 g.
- Maintain all rats at room temperature at 22 °C, with 12 hours of light and dark cycles before experiment.
- Ensure that food and water are available ad libitum.
- Perform all procedures between 6:00 a.m. and 2:00 p.m.
2. Preparing rats for surgery
- Anesthetize the rats for 30 min with isoflurane (4% for induction and 2% for maintenance) and 24% oxygen (1.5 L/min).
- Test the level of anesthesia in the rats by ensuring they do not have a pedal withdrawal reflex.
- Insert the 24-gauge catheter into the tail vein.
NOTE: Tail warming for vasodilation is not performed.- Place the rats on the table in a supine position. Use medical tape to affix all four of the rats’ limbs.
- Place the probe for temperature measurement into the rat rectum before surgery.
- During the procedure, maintain a heating plate to support a 37 °C core body temperature.
- Add ointment in both of the rat’s eyes for protection.
- Shave the surgical area and disinfect with three applications of 10% povidone-iodine followed by 70% isopropyl alcohol.
3. Right side middle cerebral artery occlusion
NOTE: MCAO is performed by a modified technique, as previously described16,22,23, with the use of instruments described by McGarry et al.24 and Uluç et al.25.
- Dissect the skin and superficial fascia at the ventral midline of neck with surgical tweezers and scissors with curved blades.
- Identify the muscle triangle, consisting of the ICA, external carotid artery (ECA) and common carotid artery (CCA).
- Carefully separate the right CCA and ICA from the vagus nerve with microforceps for vascular surgery.
- Expose the right CCA and the ICA. Block the blood flow coming from the CCA to the ICA using either micro-clips or special tourniquets for vascular surgery. Make an incision (approximately 1 mm) on the ICA using microscissors for vascular surgery.
- Insert a monofilament catheter (4-0 nylon) directly through the ICA, about 18.5-19 mm from the bifurcation point of the right CCA into the circle of Willis until reaching a mild resistance, to occlude the MCA26.
- Ligate around the ICA above the bifurcation of CCA.
- For the sham-operated control group, perform an insertion of nylon thread instead of steps 3.5 and 3.616,22.
- Administer 5 mL of 0.9% sodium chloride by intraperitoneal injection.
- Close the wound by suture and take the rat to a recovery area.
NOTE: A few minutes after the end of anesthesia, the rat will wake up and move independently around the cage. - At 23 h after MCAO, inject 2% Evans blue in saline (4 mL/kg)23,26 into the tail vein for both operated groups via a cannula27.
NOTE: This is used as a blood-brain permeability tracer. Allow to circulate for 60 minutes.
4. Determination of infarct zone
- Measure IZ at 24 h after MCAO as described previously9,15,18,19,26.
NOTE: Rats that lost more than 20% of their weight or developed seizures or hemiplegia are excluded from the experiment. - Euthanize the rat by replacing the inspired gas mixture with 20% oxygen and 80% carbon dioxide until the rat ceases to breathe spontaneously.
- Open the chest with a 5-6 cm lateral incision through the abdominal wall under the rib cage using scissors and surgical forceps.
- Perform a diaphragmatic incision along the entire length of the rib cage with scissors and surgical forceps.
- Carefully displacing the lungs, cut through the rib cage up to the collarbone on the right and left sides28.
- Perfuse with 200 mL of normal saline through the left ventricle of the heart.
- Puncture or incise the right atrium of the heart with scissors.
- Perform decapitation using a guillotine and collect brain tissue.
- Using iris scissors, cut from the foramen magnum to the distal edge of the posterior skull surface on both sides.
- Separate the olfactory bulbs, nervous connections along the ventral surface and dorsal surface of the skull from the brain.
- Remove the brain from the head.
- Produce 6 brain slices by creating 2 mm thick horizontal sections with a .009" stainless steel, uncoated, single edge razor blade.
- Incubate for 30 min at 37 °C in 0.05% TTC.
- Place the brain tissue on the microscope slides and perform optical scanning of these 6 brain-slices with a resolution of 1600×1600 dpi (see Supplement 1 for example).
- Add a blue filter with a photo editor (e.g., Adobe Photoshop CS2) using the Channel Mixer function (Image > Adjustments > Channel Mixer) and save the image as a JPEG file format.
NOTE: After applying the blue filter, the image will appear greyscale. - Open the saved image in ImageJ 1.37v29,30.
NOTE: This computer program uses a threshold function to isolate and calculate the pixels that are either black or white (see Figure 1). - For each of the 6 brain slices of the image, select and save each hemisphere (right injured ipsilateral and left uninjured contralateral) as a separate image file using the “polygon selection” tool from the main menu.
- Set the cut-off for determining IZ by using an auto threshold function from the main menu of the ImageJ software by selecting Image > Adjust > Threshold, and measure the number of pixels in each hemisphere of a single brain set.
NOTE: Macros may be used for this step in ImageJ software (see Supplement 2 for the code). The cut off is a critical parameter for determining which pixels to convert to white and which to convert to black depending on the shade of gray (see Supplement 3 and Supplement 4 as examples). ImageJ then compares white and black pixels to determine IZ. Based on the staining protocol and scanner settings, we used a constant cut-off value of 0.220. - Perform measurement of IZ correcting for tissue swelling using the Ratios of Ipsilateral and Contralateral Cerebral Hemispheres (RICH) method13,23 (see example in Supplement 5).

NOTE: Infarct size is assessed as a percentage of the contralateral hemisphere.
5. Determination of brain edema31
NOTE: Use ImageJ 1.37v for measurement of BE32,33.
- Measure BE 24 h after MCAO. For calculation of BE, use the data from left and right hemisphere volume (in units).
- Perform optical scanning with a resolution of 1600×1600 dpi (see Supplement 1 for example).
- Select brain hemispheres and set the cut-off for determining BE with ImageJ 1.37v, as described above in sections 4.17-4.19.
- Express the BE area as a percentage of the standard areas of the unaffected contralateral hemisphere, calculated by the RICH method using following equation (see example in Supplement 5)23,34.

NOTE: Extent of BE is assessed as a percentage of the contralateral hemisphere.
6. Determination of BBB disruption
- Measure BBB disruption 24 h after MCAO.
- Divide right and left hemispheres into six slices and put each one into a microcentrifuge tube.
- Homogenize each slice of the brain tissue in trichloroacetic acid, based on the calculation of 1 g of brain tissue in 4 mL of 50% trichloroacetic acid.
- Centrifuge at 10,000 x g for 20 min.
- Dilute supernatant liquid 1:3 with 96% ethanol.
- Perform luminescence spectrophotometry by utilizing spectrophotometry software, installing the plate, and performing a sample reading using the following parameters: Fluorescence intensity excitation wavelength of 620 nm (bandwidth 10 nm) and an emission wavelength of 680 nm (bandwidth 10 nm)23,35 ; Mod top; Number Flesh 25; Manual 100; Shaking 1 sec, 1 mm.
NOTE: Use an excitation wavelength of 620 nm (bandwidth 10 nm) and an emission wavelength of 680 nm (bandwidth 10 nm).23,35
Infarct zone measurement
An independent-sample t-test indicated that 19 rats that underwent permanent MCAO demonstrated a significant increase in brain infarct volume compared to the 16 sham-operated rats (MCAO=7.49% ± 3.57 vs. Sham = 0.31% ± 1.9, t(28.49) = 7.56, p < 0.01 (see Figure 2A)). The data is expressed as a mean percentage of the contralateral hemisphere ± SD.
Brain edema measurement
An independent-sample t-test indicated that 19 rats that underwent permanent MCAO demonstrated significant increase in the extent of brain edema after 24 h compared to the 16 sham-operated rats (MCAO=12.31% ± 8.6 vs. Sham = 0.64% ± 10.2, t(29.37) = 3.61, p = 0.01, d = 1.23 (see Figure 2B)). The data is expressed as a mean percentage of the contralateral hemisphere ± SD.
Blood brain barrier permeability
An independent-sample t-test indicated that 19 rats that underwent permanent MCAO demonstrated significant increase in the extent of BBB breakdown after 24 h compared to the 16 sham-operated rats (MCAO=2235 ng/g ± 1101 vs. Sham = 94 ng/g ± 36, t(18.05) = 8.47 p < 0.01, d = 2.7 (see Figure 2C)). The data are measured in ng/g of brain tissue and presented as mean ± SD.
| Group | Time | Procedures |
| Sham operated (16 rats) | 0 | Induction of MCAO and insertion of filament for sham operated group |
| MCAO (19 rats) | ||
| Sham operated (16 rats) | 23h | Injection of Evans blue |
| MCAO (19 rats) | ||
| Sham operated (16 rats) | 24h | Brain collection for measurements of IZ, BE, and BBB disruption |
| MCAO (19 rats) |
Table 1: Protocol timeline. At 23 h after MCAO, the Evans blue solution was injected. One hour later (24 h after MCAO), brain collection was performed, and IZ, BE and BBB permeability were measured in all groups.
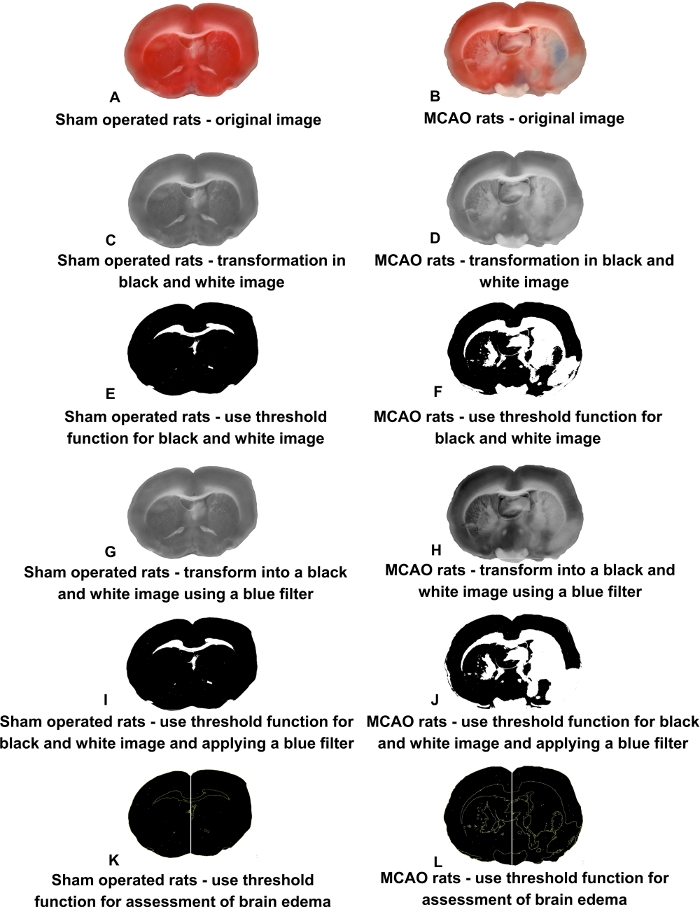
Figure 1: Representative brain slices of sham-operated and MCAO rats.
(A-B) Original scanned image. (C-D) Transformation to greyscale. (E-G) Threshold function. (G-H) Application of a blue filter. (I-J) Threshold function after blue filter application. (K-L) Using threshold function to assess brain edema. Please click here to view a larger version of this figure.
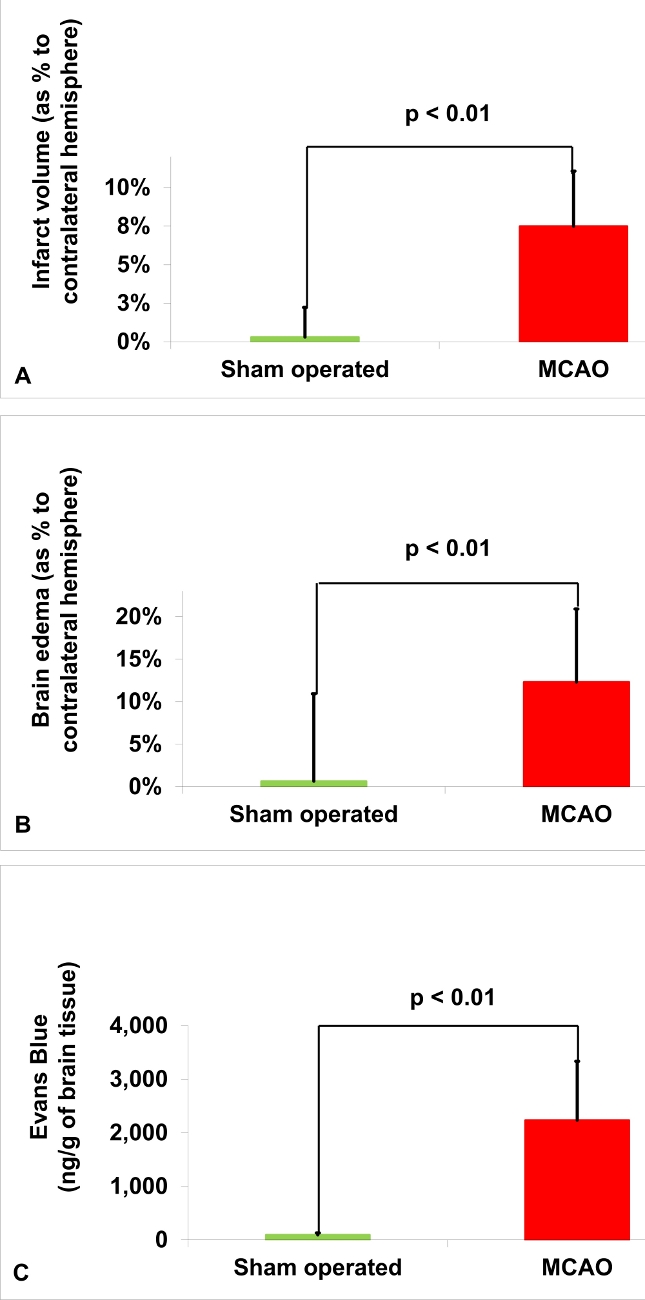
Figure 2: Histological outcomes of MCAO rats compared to sham-operated rats.
(A) Infarct zone. The infarct zone volume in 19 rats after MCAO was significantly increased compared to the 16 sham-operated rats 24 h after surgery (*p < 0.01). (B) Brain edema. The brain edema volume in 19 rats after MCAO was significantly increased compared to the 16 sham-operated rats 24 h after surgery (*p < 0.01). (C) Blood brain barrier permeability. The blood brain barrier permeability in 19 rats after MCAO was significantly increased compared to the 16 sham-operated rats 24 h after surgery (*p < 0.01). Values were expressed as a mean percentage of the contralateral hemisphere ± SD and mean Evans blue extravasation index in ng/g of brain tissue ± SD according to independent-samples t-test. Results were considered statistically significant when p< 0.05, and highly significant when p < 0.01. This figure has been modified from Kuts et al.23 Please click here to view a larger version of this figure.
Supplement 1: Example scan of brain slices. Please click here to download this figure.
Supplement 2: Macros that may be used in ImageJ software for the auto threshold function and measuring pixels. Please click here to download this file.
Supplement 3: Example auto threshold. Please click here to download this figure.
Supplement 4: Example of measured pixels on each hemisphere. Please click here to download this figure.
Supplement 5: Sample analysis. Please click here to download this figure.
