Participants
Participants were recruited from local high school teams and university intercollegiate and club sports teams using word-of-mouth and advertising flyers. Participants were required to be between the ages of 15-22 and engage in regular participation in organized contact sports. Contact sports included all sports where physical contact with teammates or opponents is necessary during routine play. Participants also had to have normal or corrected vision and hearing, no history of neurological or psychiatric conditions, and no history of moderate or severe traumatic brain injury, per self-report.
We included data from three healthy male contact-sport athlete participants (Mean Age: 18.0 ± 2.65 yrs.) to illustrate the type of clinical data that can be acquired from the revised DTS. Data from healthy, female contact-sport athletes will be included in another publication that is not strictly Methods-focused.
Data Analysis for Revised DTS
Given the small number of participants included in the representative results, formal statistical analyses were not completed. However, for each participant, performance in the dual task condition was compared to performance in the single motor and single cognitive conditions; see below for the description of the performance metrics on both subtasks.
Performance Metrics on the LE Subtask
Single motor condition performance was quantified by gait speed (m/s), total number of steps, average step length (m), average step duration (s), and variability of step duration (SD). These data were acquired with the built-in accelerometers on the smart devices we affixed to participants’ ankles. Single cognitive condition performance was measured by the total number of words produced without repetitions, represented as words/s to account for the varied amount of time allotted for this trial. Two trained research assistants watched a video tape of the single cognitive condition and were required to reach a consensus on the total number of words produced. Finally, dual task condition performance was measured by gait speed (m/s), total number of steps, average step length (m), average step duration (s), and average step duration variability (SD), and the total number of words produced without repetitions, represented as words/second. Two trained research assistants also watched a video tape of the dual task condition and were required to reach a consensus on the total number of words produced.
Dual Task Costs on the LE Subtask
For each participant, a dual task motor cost would be represented by the following changes in gait characteristics during the dual task condition compared to the single motor condition: slower gait speed, a greater number of total steps, a smaller average step length, a longer average step duration, and a greater step duration variability. We observed that all three male participants had a dual task motor cost on the LE Subtask. Specifically, we saw slower gait speed, longer average step duration, and greater variability in step duration during dual, compared to single condition tasks; see Figure 1A. In contrast, two of three participants showed no changes in number of total steps or average step length between single motor and dual task conditions; see Figure 1A.
For each participant, a dual task cognitive cost would be represented by fewer words generated in the dual task condition compared to the number of words generated in the single cognitive task condition. We observed dual task cognitive costs in two of three participants. Specifically, these participants generated fewer words during the dual task condition compared to the single task condition; see Figure 1B.
Performance Metrics on the UE Subtask
Single motor condition performance was measured by the total number of successful catches. Two trained research assistants watched a video tape of the single motor condition and were required to reach a consensus on the total number of successful catches. Single cognitive condition performance was measured by the total number of correct subtractions. Two trained research assistants watched a video tape of the single cognitive condition and were required to reach a consensus on the total number of correct subtractions. Subtraction errors were not cumulative (i.e., “100, 92, 85…” would be recorded as one error and one correct subtraction). Finally, dual task condition performance was measured by the total number of successful catches and total number of correct subtractions. Again, two trained research assistants watched a video tape of the single cognitive condition and were required to reach a consensus on the total number of successful catches and correct subtractions.
Dual Task Cost on the UE Subtask
For each participant, a dual task motor cost would be represented by fewer successful catches during the dual task condition compared to the number of successful catches made during the single motor condition. We found that all three male participants had a dual task motor cost. Specifically, they had fewer successful catches during the dual task condition compared to the single motor condition; see Figure 2A.
A dual task cognitive cost would be represented by fewer correct subtractions the dual task condition compared to the number of correct subtractions made during the single task condition. We observed dual task cognitive costs in two of three participants. Specifically, they had fewer correct subtractions during the dual task condition compared to the single task condition; see Figure 2B.
Data Analysis for Neuroimaging-Compatible DTS
fNIRS Device Specifications
We used a mobile functional near-infrared spectroscopy (fNIRS) system (Table of Materials). The system has 32 total optodes, 16 LED sources and 16 detectors, and a wireless acquisition device that participants wear on their backs. This device is uniquely equipped to accommodate gross motor movement, and has (to our knowledge) the greatest amount of head coverage for a mobile system. Using fNIRS we evaluated brain activity via the hemodynamic response using indices of oxygenated hemoglobin (HbO) during the neuroimaging-compatible DTS.
fNIRS Head Probe
The head probe included 30 optodes (15 LED sources and 15 detectors) that were placed on the participant’s head using an fNIRS cap with built-in optode holders. We measured HbO by placing LED sources and detectors at the left and right motor cortex and two primary regions of the right-lateralized frontoparietal network16, right PFC and PPC, which we have identified with the 10-20 system17; see Figure 3. The LED sources shine near-infrared light into superficial cortical regions, and the detectors capture the refracted light, allowing us to calculate HbO values at each channel, or intersection of source and detector. Additionally, we include eight short separation detectors, which measure scalp perfusion, a nuisance variable that will be regressed out of the raw fNIRS data18,19.
Block Design for fNIRS Acquisition
Both the LE and UE subtasks were converted into a block design. Both subtasks started and ended with a 60 s seated rest period to acquire baseline hemodynamic activity. Rest was followed by 15 randomized blocks (5 single motor condition blocks, 5 single cognitive condition blocks, and 5 dual task condition blocks) that were 30 s in duration, totaling 7.5 minutes of total data collection for each subtask. Between each of the 15 condition blocks, there was a variable resting interval of approximately 6-8 s to allow the participants’ hemodynamic response to return to baseline; see Figure 4.
FNIRS Data Reduction and First-Level (Single-Subject) Analysis: Raw fNIRS data are uploaded into a proprietary programming language and numerical computing environment (Table of Materials). Channels created with short separation detectors are labeled for later regression. Default stimuli values, which were generated by the stimulus presentation software, are renamed to identify DTS blocks (e.g., single motor, single cognitive, dual motor). Next, stimulus duration parameters are set to 30 seconds for all DTS blocks and 60 s for rest periods. Basic processing is then completed using steps from a non-proprietary toolbox that is compatible with the numerical computing environment. These steps include calculating optical density and then recalculating optical density values given data from the short separation channels20. Next, optical density is converted to hemoglobin values (deoxygenated hemoglobin, oxygenated hemoglobin, and total hemoglobin) using the modified Beer Lambert Law21. Following conversion, an autoregressive model algorithm is run, which includes regression of short separation channel data. Parameters for the autoregressive algorithm are set to follow a Canonical model22. Finally, individual data can be visualized using condition contrasts (e.g. Dual vs Single); see Figure 5.
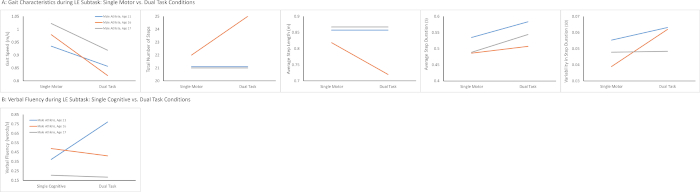
Figure 1: LE Subtask Performance during Single vs. Dual Task Conditions. (A) All three participants had slower gait speed, longer average step duration, and greater variability in step duration during the dual task condition compared to the single task condition, which represents a dual task motor cost on the UE subtask. Two of three participants showed no changes in number of total steps or average step length between dual and single task conditions. (B) Two of three participants generated fewer words during the dual task condition compared to the single task condition, which represents a dual task cognitive cost on the LE subtask. Please click here to view a larger version of this figure.
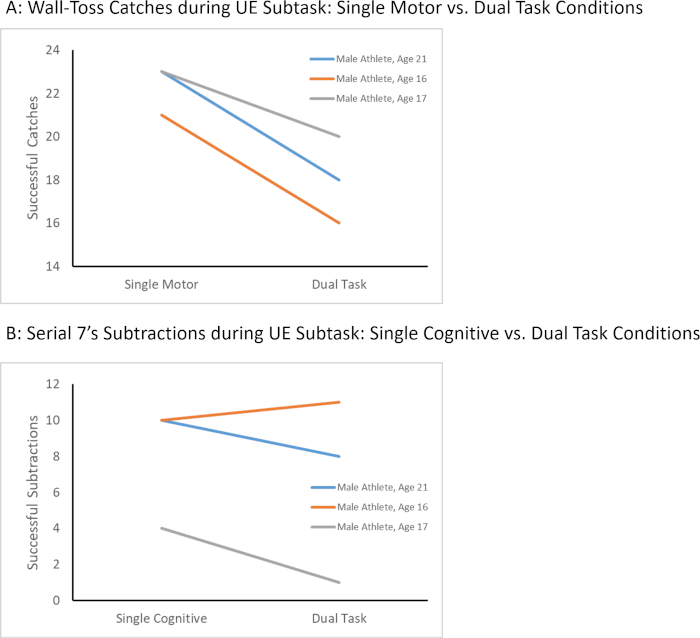
Figure 2: UE Subtask Performance during Single vs. Dual Task Conditions. (A) All three participants had fewer successful catches during the dual task condition compared to the single task condition, which represents a dual task motor cost on the UE subtask. (B) Two of three participants had fewer correct subtractions during the dual task condition compared to the single task condition, which represents a dual task cognitive cost on the UE subtask. Please click here to view a larger version of this figure.
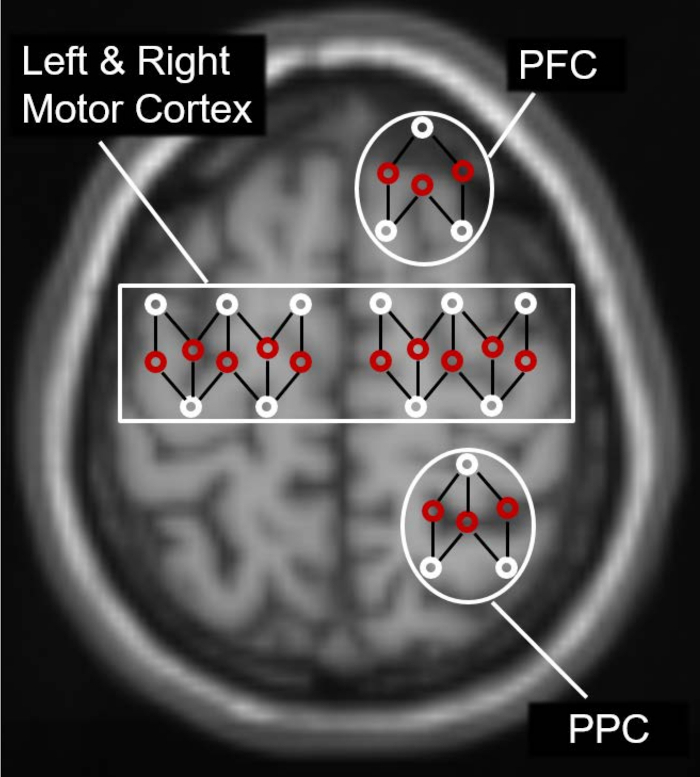
Figure 3: FNIRS Head Probe. The fNIRS head probe included 15 LED sources (red circles) and 15 detectors (white circles) which were placed at the left and right motor cortex and right prefrontal cortex (PFC) and right posterior parietal cortex (PPC). This allowed us to calculate oxygenated hemoglobin (HbO) values at each channel, or intersection of source and detector. Please click here to view a larger version of this figure.
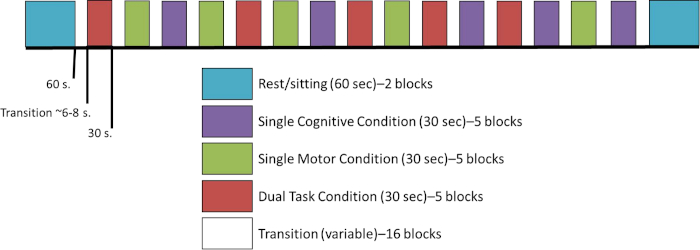
Figure 4: Block Design for fNIRS Acquisition. For the neuroimaging compatible version of the DTS, the LE and UE subtasks were converted into a block design. Both subtasks started and ended with a 60 second seated rest period to acquire baseline hemodynamic activity. Rest was followed by 15 randomized blocks (5 single motor condition blocks, 5 single cognitive condition blocks, and 5 dual task condition blocks) that were 30 seconds in duration. Please click here to view a larger version of this figure.
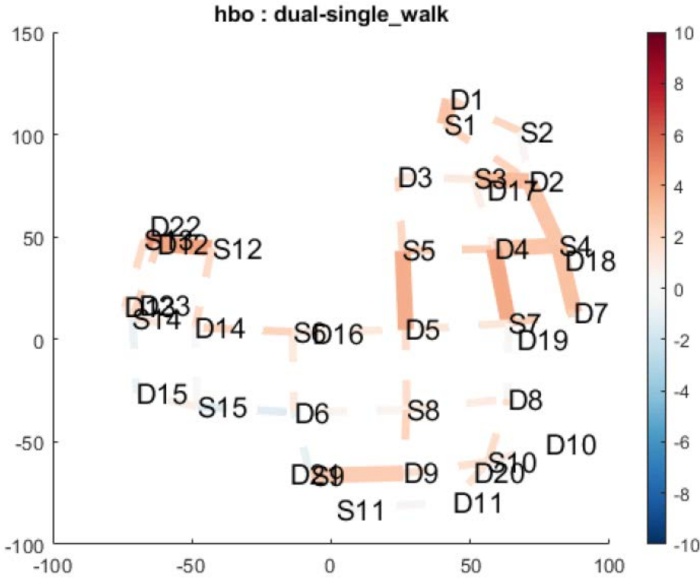
Figure 5: Single Subject fNIRS Data. This is a depiction of single subject fNIRS data using condition contrasts. This image contrasts oxygenated hemoglobin (HbO) during the Dual Task vs Single Motor Task from the LE subtask. Please click here to view a larger version of this figure.
