The protocol outlined in this study highlights the details of venous clot modeling, lysotripsy for clot disruption, and ultrasound imaging in an in vitro setup of DVT. The adopted procedure demonstrates the steps necessary to assess clot disruption due to the combined effects of rt-PA and histotripsy bubble cloud activity. The benchtop setup was designed to mimic the characteristics of a venous iliofemoral vein. Figure 1A shows a model vessel that has the acoustic, mechanical, and geometrical properties of the iliofemoral vein. The clot is placed inside the model vessel to mimic a partially occlusive thrombus. The clot is perfused with plasma and rt-PA drawn from a reservoir at a rate of 0.65 mL/min. This rate is consistent with slow flow rate in a highly occluded vessel34.
An elliptically focused transducer of 1.5 MHz fundamental frequency with a 9 cm major axis, 7 cm minor axis, and 6 cm focal length (Figure 2A) is mounted on the positioning system as noted in Figure 1B. An imaging array covered with ultrasound gel and a latex cover (Figures 2B,C) is mounted coaxially with the transducer as shown in Figure 1A via an opening in the center of the histotripsy source. The motorized positioners were used to translate the therapy transducer/imaging array along the clot length within the model vessel (Figure 1). Upon application of sufficient voltage to the histotripsy source, a bubble cloud is generated in the focal region of the transducer and visualized via ultrasound imaging, as shown in Figure 3. The focal position is defined as the center of the bubble cloud using the imaging plane (steps 4.10-4.11).
Figure 4A shows perfusates collected for two different treatment conditions. The beaker labeled as control contains perfusate of a clot exposed to plasma alone. The second beaker labeled as treated contains the perfusate of the lysotripsy treated clot. The collected perfusates are used to assess the hemoglobin (metric of hemolysis) and D-dimer (metric of fibrinolysis) content through assays as specified in the protocol. The difference in color of the perfusates denotes variability in hemoglobin concentration, which can be quantified via optical absorbance. The relationship between absorbance value and hemoglobin concentration can be determined through a calibration curve. Solutions with known hemoglobin content ranging from 0 (blank measurement) to 180 mg/mL are placed in the well plate and absorbance is determined in triplicate using the plate reader (Figure 4B,C). The upper absorbance limit of the plate reader may vary and may not be known a priori to making the solutions in the well plate. As such, hemoglobin concentrations up to 180 mg/mL are made in the well plate, Figure 4B. However, the plate reader used here can read absorbance for concentrations up to 23 mg/mL only, Figure 4C.
Figure 5A shows visualization of the clot within the model vessel via B-mode imaging prior to histotripsy exposure as specified in step 7.2.3. This image is acquired to determine the clot position for segmentation of the passive cavitation image. Figure 5B shows the passive cavitation image co-registered with the B-mode image acquired prior to histotripsy exposure. This figure confirms that acoustic energy is contained primarily within the clot during histotripsy exposure.
Typical clot disruption due to histotripsy and lytic are indicated in Figure 6. Figure 6A,B show the untreated and lysotripsy treated clot images, respectively. For samples exposed to histotripsy, disruption is primarily restricted to the clot center, consistent with the observed locations of bubble activity tracked with passive cavitation imaging (Figure 5B). However, with addition of lytic, mass loss also occurs in regions closer to the periphery of the clot. It is hypothesized that this additional mass loss is due to enhanced fluid mixing of the lytic under bubble activity. Fluid mixing increases the distribution and penetration depth of the lytic into the clot. Since the lytic is responsible for fibrinolysis40, the mass loss increases. Fibrinolysis can be quantified by measuring the D-dimer content in the perfusate41.
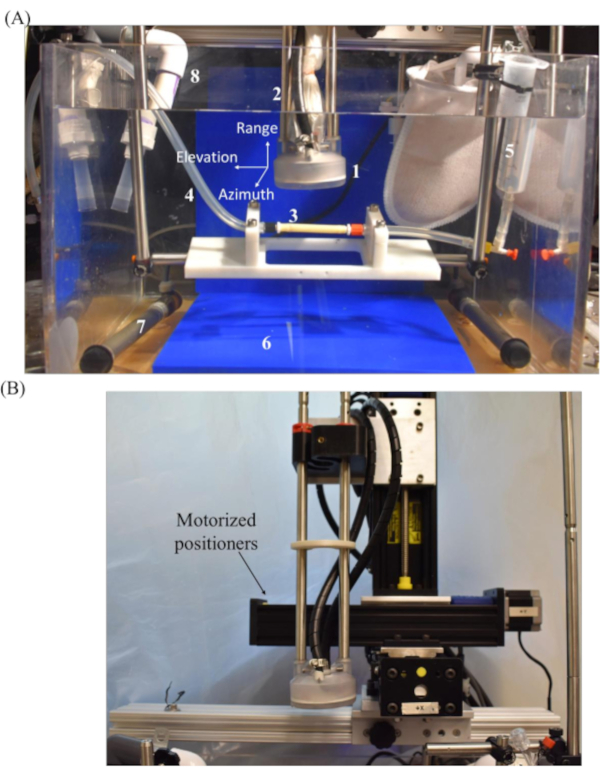
Figure 1: Experimental setup for lysotripsy of human blood clot. (A) The components of the setup are (1) focused histotripsy source with elliptical geometry, (2) latex-covered imaging array, (3) model vessel attached to flow channel, (4) flow channel, (5) reservoir, (6) acoustic absorbing material, (7) heating element, and (8) water tank filled with degassed and heated reverse osmosis water. The azimuth dimension of the imaging plane is perpendicular to the elevational and range dimensions (into the page). (B) The histotripsy source mounted on the motorized positioning system. Please click here to view a larger version of this figure.
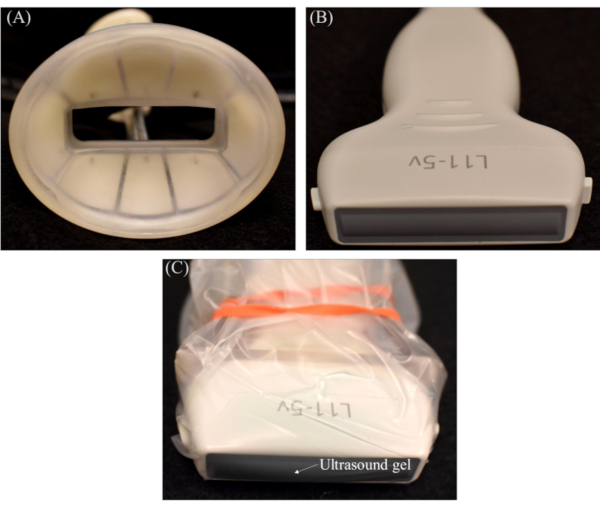
Figure 2: Ultrasound source and imaging components. Individual zoomed images of (A) focused histotripsy source, (B) imaging array, and (C) imaging array with ultrasound gel and latex cover. Please click here to view a larger version of this figure.
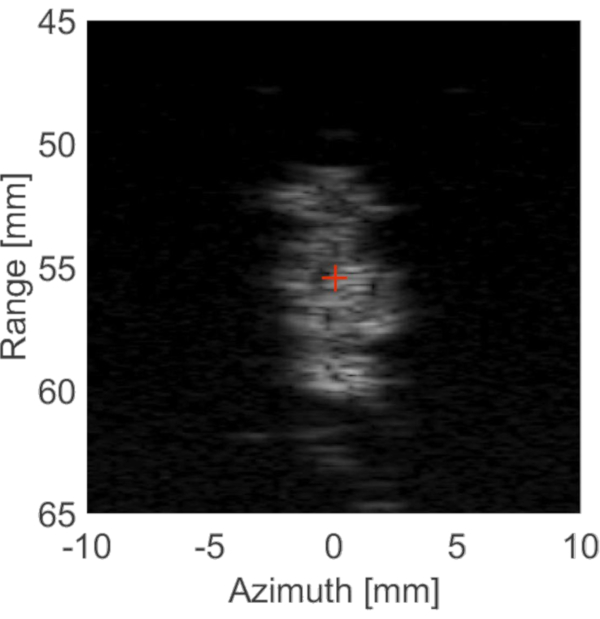
Figure 3: Histotripsy bubble cloud visualized using imaging array. A bubble cloud is generated in the focal zone of the histotripsy source and imaged using an imaging array. The designated focus, shown as a cross, is saved for treatment planning. Please click here to view a larger version of this figure.
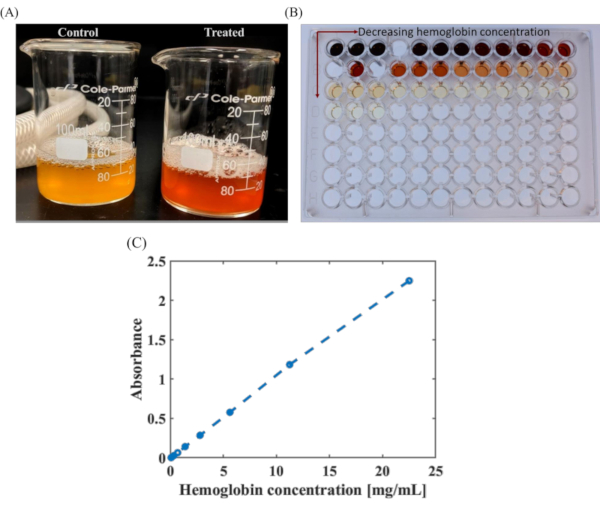
Figure 4: Quantification of hemoglobin released due to clot lysis. (A) Perfusate samples collected following control study with plasma alone (no histotripsy or lytic), and treatment arm, histotripsy (e.g., 35 MPa peak negative pressure, 5 cycle pulse duration, 1.5 MHz fundamental frequency), and 2.68 µg/mL lytic exposure. (B) Well plate containing dilutions of known hemoglobin concentrations ranging from 180 mg/mL (top row, left-most corner) to 0 mg/mL (bottom row, right-most corner). The arrowhead points toward decreasing hemoglobin concentration. (C) These samples are used to create a standard curve to quantify hemoglobin produced due to histotripsy exposure via spectrophotometry. Absorbance curve for hemoglobin concentrations ranging from 0 to 23 mg/mL is obtained due to limitation of the plate reader in analyzing higher concentrations. Please click here to view a larger version of this figure.
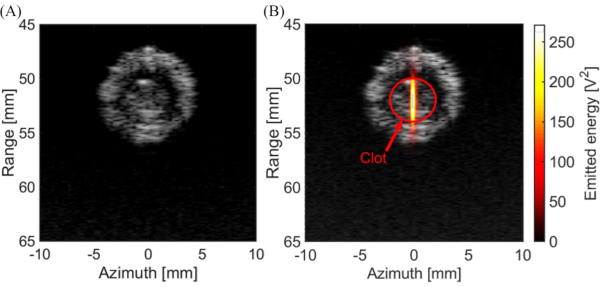
Figure 5: Images of the clot during treatment. (A) B-mode image acquired before the start of treatment pulse showing the clot position within the model vessel. (B) Post-hoc visualization ofacoustic energy emission calculated from passive cavitation imaging shown in hot colormap co-registered with B-mode image of the clot acquired prior to application of the histotripsy pulse. Please click here to view a larger version of this figure.
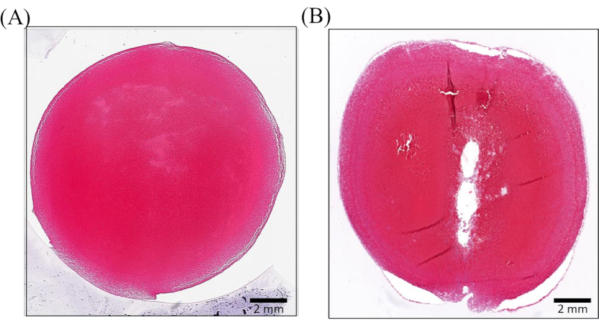
Figure 6: Histology of the ablated clot under different treatment conditions. (A) Control clot without treatment. (B) Clot treated with lysotripsy (e.g., 35 MPa peak negative pressure, single cycle pulse duration, 1.5 MHz fundamental frequency). The histotripsy pulse propagated from top to bottom in this image. The path for the histotripsy source along the length of the clot (i.e., perpendicular to the plane of the image shown here) is defined in step 7.2.3. The scale of the micrographs is 2 mm. Note that the degree of clot disruption achieved here would be reduced compared to insonation schemes with longer pulse duration24. Please click here to view a larger version of this figure.
