All animal experiments described were approved by the University of Michigan's Committee on the Use and Care of Animals.
1. Tissue harvest
- Euthanize mice humanely using isoflurane anesthesia followed by cervical dislocation, in accordance with approved protocols. For all animal experiments, approval was obtained by a certified review board in accordance with the National and Institutional guidelines for animal handling.
- Place the mouse on a dissecting pad in a supine position. Immobilize mouse extremities using 20 G x 1 1/2-inch G needles.
- Using forceps and scissors, make a small incision on the abdominal skin and pull it to the side to expose the peritoneum.
- Open the abdominal cavity with a midline incision in the peritoneum from the pubic bone to the sides of the abdomen.
- Carefully remove tissues and organs until large intestine is visualized. Cut the pelvic bone on both sides of the colon to fully visualize the organ, extending from the anus towards the cecum.
- Gently remove fat, small veins and arteries attached to the colon, while carefully dissecting the organ, cutting just proximal to the anus and just distal to the cecum.
NOTE: The dissected colon should remain at room temperature while completing the Swiss roll procedure. - Carefully flush the colon with 1x PBS, using a flexible plastic gavage needle inserted through the anus to remove fecal contents.
- Position the colon in a straight line, and open longitudinally along the mesenteric artery. Bisect the colon longitudinally from the distal to the proximal end (Figure 1A). One half of the tissue can be used for histological analysis while the other can be processed for western blot, PCR or rolled into a second Swiss roll for fresh frozen immunofluorescence microscopy12.
2. Preparation of swiss rolls
- Trim extra tissue from the proximal colon using a razor blade until approximately the same width along the length of the whole colon is obtained.
- Align the colon to expose the lumen facing-up, and flatten the tissue completely using a flexible gavage needle. Add more PBS, if needed, to keep the tissue moist throughout the procedure.
- Remove the excess of PBS using a paper wipe. With a syringe and gavage needle, add 10% neutral buffered formalin solution over the tissue for 2-3 min to fix and flatten the tissue.
- Use straight forceps to grab the end of the distal colon and twist the colon into concentric circles from the distal to proximal end (Figure 1B).
NOTE: It is possible to push back the inside of the Swiss roll while rolling using the forefinger to ensure the tissue is inside the roll. - Insert a 27 G needle to pin the colon in the middle to hold its Swiss roll shape (Figure 1C).
- Place the Swiss roll with the needle into an embedding cassette inside a histologic specimen container.
NOTE: Tissue must be oriented in parallel with respect to the cassette before fixation (Figure 1D). - Fix the tissue in 10% neutral buffered formalin solution overnight at 4 °C13.
- After overnight fixation, wash the tissue 3x with PBS.
- Add 70% ethanol to the tissue prior to the paraffin embedding process. Remove the needle from the Swiss roll before proceeding. Tissue can be stored in ethanol at room temperature until paraffin embedment13.
- Place samples into the tissue processor, embed in paraffin, and prepare 4 µm sections, mounted on positively charged microscopy slides (Figure 1E). This can be an optional stop point.
NOTE: Proper tissue orientation is critical to achieve sections suitable for image analysis. Parallel Swiss roll embedding in the paraffin cassette will result in full sections appropriated for image analysis (Figure 1F-1H). Oblique sections must be avoided to prevent incomplete sections (Figure 1I-1K). For more details, see the Discussion section. - Stain sections with hematoxylin and eosin (H&E)13.
3. Digital scanning and analysis
NOTE: For accurate evaluation of mucosal changes, select only sections that include at least 90% of the total colon length.
- Scan stained sections using a slide scanner or imager (see Table of Materials). Images produced need a resolution of 0.25 microns per pixel with 40x objective and 40x magnification.
- Install and download an appropriate software for digital analysis of scanned slides (see Table of Materials).
- Open scanned images in the image processing software (Figure 2A). Verify that the entire colon is visible and that there are no missing areas of the sample.
- Activate the label imager and scale bar tools to properly identify scanned slides by clicking Label imager (Figure 2A).
- Open the annotations tool by clicking Annotations, (Figure 2A) and create 3 different layers by clicking New layer (Figure 2B) to quantify the total length the Swiss roll, inflammation/injury, and erosion/ulceration. Choose a different color for each layer by clicking Layer color (Figure 2B).
- Measure the length of each layer/category by clicking the Pen tool (Figure 2A), using the muscularis mucosa as a reference:
- View the image at 400 µm zoom (or more) to facilitate adequate visualization of the muscularis mucosa.
NOTE: Magnification is easily controlled using the mouse scroll wheel and will need to be adjusted as necessary while moving across the section to draw all the lines. - Click on the Pen tool to draw a line following the muscularis mucosa (Figure 2A). Move the pointer as needed to visualize the adjacent area for analysis.
NOTE: Each time that the pen is stopped, a small new layer region will be generated. It can be visualized and edited with the Layer regions tab (select desired segment and click Delete Layer in case of mistakes or corrections, Figure 2B).
- View the image at 400 µm zoom (or more) to facilitate adequate visualization of the muscularis mucosa.
- Once all layers (Figure 2C) are defined, export the data using the Export Grid to Text File button inside the layer regions options (Figure 2B).
NOTE: Save files often while creating the layers to ensure data is properly stored. - Open the text files and copy the data with a spreadsheet software. Total all the segments from each region and calculate percentage of injury and ulceration with respect to total length.
- To calculate the Histological Colitis Score (HCS) and to evaluate the severity of disease, consider three main characteristics as detailed below.
- Check for healthy intestinal mucosa which is characterized by organized epithelial cells in the crypt-luminal axis, lamina propria with few immune cells, and subjacent muscularis mucosa that interfaces the mucosa and submucosa (Figure 3A).
- Check for inflammation/injury which is characterized by epithelial crypts that are attenuated or partially missing epithelial cells and mucosal inflammation with neutrophil infiltration into crypts (Figure 3B).
- Check for the presence of erosion/ulceration which is characterized by areas devoid of surface epithelium or areas completely lacking epithelial crypts with or without associated leukocytes (Figure 3C).
- Calculate HCS of injured and ulcerated regions expressed as a percentage of the total length in the following formula:

NOTE: HCS combines the percentage of inflammation/injury and erosion/ulceration adding a factor of two to the latter, based on a reasonable assumption that complete loss of the epithelium results in maximum loss of barrier integrity and hence worse disease. HCS consistently represents the morphological changes caused by DSS induced experimental colitis. Interestingly, we have not seen a clear correlation between the numbers of colonic lymphoid aggregates or follicles and clinical disease severity in DSS colitis and, therefore, we did not include the quantification in this analysis. - Take a snapshot of the representative images (click Snapshot, Figure 2A), and save. Include scale bars if needed by clicking on Show/Hide Scale Bar (Figure 2A).
To illustrate the reliability of this Histological Colitis Score Analysis in the context of mucosal damage after DSS challenge and subsequent recovery from colitis, we administered 2.5% DSS in the drinking water of eight 10 weeks old male C57BL6 wild type mice for 5 days followed by a recovery period with regular water for 5 days. There was no change in body weight during the acute administration of DSS, from day 0 to 5 (Figure 4A). Body weight dramatically decreased after day 5, when mice started drinking regular tap water. Blood and soft stools appeared after 3 days of DSS administration and continued for the subsequent 3 days on water until day 8 of the experiment (Figure 4B). These observations suggested that the most detrimental effects of exposure to DSS were observed during the recovery period between days 5 and 8. Measurement of the colon length on the day 10 confirmed a significant shortening at the end of the experiment (Figure 4C). Colons were harvested at days 0, 2, 5, 7, 8, and 10 to make paraffin Swiss rolls. Tissue was stained with H&E and high-definition scans (Figure 4D) were analyzed to calculate the Histological Colitis Score (Figure 4E) and percentage of injury and ulceration (Figure 4F).
Figure 4D shows normal crypt architecture in untreated C576BL6 mice, superficial to the muscularis mucosa and supported by the lamina propria (day 0, arrow). After 2 days of DSS administration, immune cell recruitment was observed (day 2, arrow). On day 5, epithelial cells appeared damaged, and there was an infiltration of neutrophils across the epithelium (cryptitis) associated with epithelial injury (day 5, arrow). From day 5 to 8, areas of epithelial loss with inflammation and ulceration were noted (day 7 and 8, arrows). The latter is commonly observed as the mice drink regular tap water during the recovery phase. Finally, epithelial cells begin to regenerate and repopulate ulcerated areas, slowly restoring colonic mucosa at day 10 (arrow).
HCS closely mirrors simple assessment of percentage of inflammation/injury and erosion/ulceration, and both quantitatively demonstrate that there is significant damage to the colon of mice during recovery from DSS on day 5 to 10, which correlates with epithelial erosions and leukocyte infiltration shown in Figure 4D. Data provided by HCS distinguishes between the severity of the disease with regards to inflammation associated with epithelial injury versus erosion/ulceration.
These observations demonstrate that the systematic scoring system of HCS proposed in this protocol constitutes a reliable tool to quantify mucosal damage.
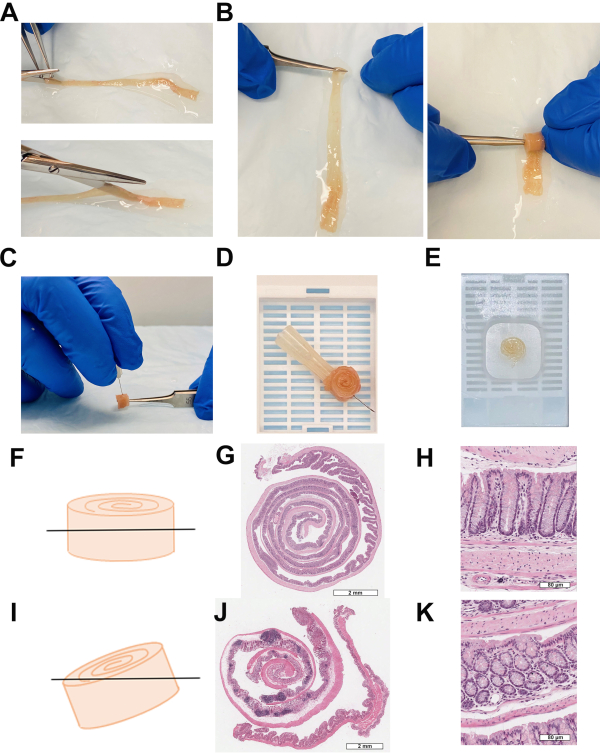
Figure 1: Sample preparation is crucial for accurate data analysis. (A) Distal colon fully extended and opened along the mesenteric artery. (B) Swiss rolling process. (C) Needle insertion to hold Swiss roll shape (D) paraffin embedding cassette. (E) Paraffin block. (F) Swiss roll parallel orientation to avoid partial sections. (G) Complete Swiss roll, scale bar: 2 mm. (H) Ideal section of colonic crypts, scale bar: 80 µm. (I) Oblique Swiss roll orientation. (J) Incomplete Swiss roll, scale bar: 2mm. (K) Oblique section of colonic crypts, scale bar: 80 µm. Please click here to view a larger version of this figure.
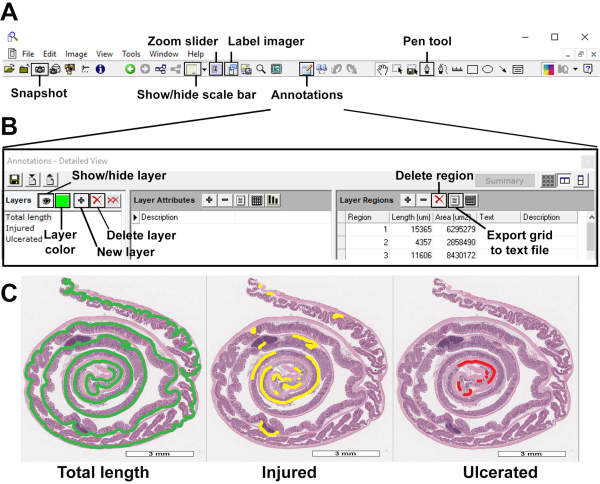
Figure 2: Quantitative evaluation of mucosal damage. (A) Basic tool bar with Snapshot, zoom slider, show/hide scale bar/axes/grid, label imager, annotations, and pen tool features, among others. (B) Annotations menu displaying layer color, new layer, delete layer, show/hide layer, delete region and export grid to text file buttons. (C) Overview of total length, injured and ulcerated layers, scale bar: 3 mm. Please click here to view a larger version of this figure.
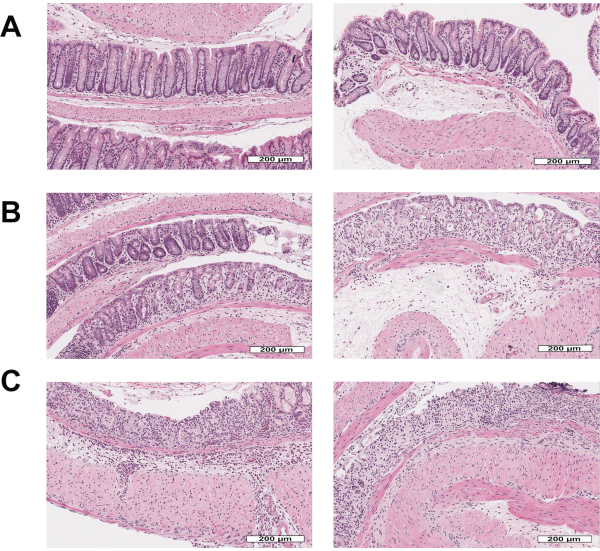
Figure 3: Morphology of mouse intestinal mucosa stained with hematoxylin & eosin after acute DSS-experimental colitis followed by recovery. (A) Healthy intestinal cells organized in colonic crypts surrounded by lamina propria and separated from the submucosa by the muscularis mucosa, scale bar: 200 µm. (B) Acute mucosal inflammation or injury with infiltration of neutrophils into the mucosa and crypt epithelium, associated with crypt epithelial distortion/loss and epithelial attenuation, scale bar: 200 µm. (C) Ulcerated or eroded areas with complete epithelial loss and associated inflammation., scale bar: 200 µm. Please click here to view a larger version of this figure.
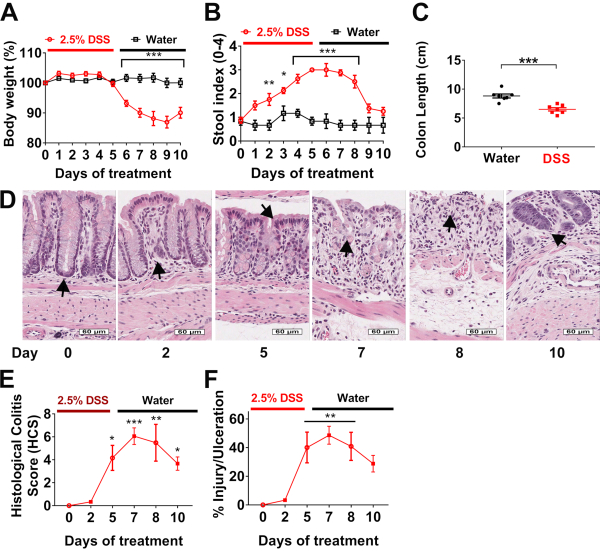
Figure 4: Histological Colitis Score and percentage of injury and ulceration correlates with body weight and stool index during DSS experimental colitis: (A) Body weight and (B) stool indexes are evaluated daily in wild type mice treated with 2.5% DSS for 5 days (red line), followed by 5 days of recovery on water (black line). Data are representative of two independent experiments with at least 4 mice per group and are expressed as mean ± SEM. Significance is determined by two-way ANOVA and Sidak multiple comparison, *p<0.033, **p<0.002, and ***p<0.001. (C) Colon length of mice was measured at day 10. Data are representative of two independent experiments with at least 3 mice per group and are expressed as mean ± SEM. Significance is determined by two-tailed Student's t test, ***p<0.001. (D) Hematoxylin and eosin (H&E)-stained tissue sections of colonic mucosa were analyzed to calculate, scale bars: 60 µm. (E) Histological Colitis Score (HCS) and percentage of injury/ulceration relative to the length of the colon. Data are representative of two experiments with 2 mice per group and are expressed as mean ± SEM. Significance is determined by one-way ANOVA and Tukey multiple comparison, *p<0.033, **p<0.002, and ***p<0.001. Please click here to view a larger version of this figure.
