Modeling Brain Metastasis Via Tail-Vein Injection of Inflammatory Breast Cancer Cells
Summary
We describe a xenograft mouse model of breast cancer brain metastasis generated via tail-vein injection of an endogenously HER2-amplified inflammatory breast cancer cell line.
Abstract
Metastatic spread to the brain is a common and devastating manifestation of many types of cancer. In the United States alone, about 200,000 patients are diagnosed with brain metastases each year. Significant progress has been made in improving survival outcomes for patients with primary breast cancer and systemic malignancies; however, the dismal prognosis for patients with clinical brain metastases highlights the urgent need to develop novel therapeutic agents and strategies against this deadly disease. The lack of suitable experimental models has been one of the major hurdles impeding advancement of our understanding of brain metastasis biology and treatment. Herein, we describe a xenograft mouse model of brain metastasis generated via tail-vein injection of an endogenously HER2-amplified cell line derived from inflammatory breast cancer (IBC), a rare and aggressive form of breast cancer. Cells were labeled with firefly luciferase and green fluorescence protein to monitor brain metastasis, and quantified metastatic burden by bioluminescence imaging, fluorescent stereomicroscopy, and histologic evaluation. Mice robustly and consistently develop brain metastases, allowing investigation of key mediators in the metastatic process and the development of preclinical testing of new treatment strategies.
Introduction
Brain metastasis is a common and deadly complication of systemic malignancies. Most brain metastases originate from primary tumors of the lung, breast or skin, which collectively account for 67-80% of cases1,2. Estimates of the incidence of brain metastasis vary between 100,000 to 240,000 cases, and these numbers may be underestimates because autopsy is rare for patients who died of metastatic cancer3. Patients with brain metastases have a worse prognosis and lower overall survival relative to patients without brain metastases4. Current treatment options for brain metastases are largely palliative and fail to improve survival outcomes for most patients5. Thus, brain metastasis remains a challenge, and the need remains pressing to better understand the mechanisms of brain metastasis progression to develop more effective therapies.
The use of experimental models has provided important insights into specific mechanisms of breast cancer metastatic progression to the brain and allowed evaluation of the efficacy of various therapeutic approaches6,7,8,9,10,11,12,13,14,15,16. However, very few models can accurately and fully recapitulate the intricacies of brain metastasis development. Several experimental in vivo models have been generated via inoculation of cancer cells into mice by different routes of administration, including orthotopic, tail-vein, intracardiac, intracarotid arterial, and intracerebral injections. Each technique has advantages and disadvantages, as reviewed elsewhere3. None of these mouse models, however, can fully replicate the clinical progression of brain metastasis.
Brain metastases are particularly common in patients with inflammatory breast cancer (IBC), a rare but aggressive variant of primary breast cancer. IBC accounts for 1% to 4% of breast cancer cases, but it is responsible for a disproportionate 10% of breast cancer-related deaths in the United States17,18. IBC is known to rapidly metastasize; indeed, one-third of IBC patients have distant metastasis at the time of diagnosis19,20. Specific to brain metastasis, patients with IBC have a higher incidence of brain metastasis than do patients with non-IBC21. Recently, we demonstrated that the MDA-IBC3 cell line, derived from the malignant pleural effusion fluid of a patient with ER–/PR–/HER2+ IBC that recapitulates IBC characteristics in mouse xenografts, has an enhanced propensity to develop brain metastases rather than lung metastases in mice when injected by tail-vein, making this cell line a good model for studying the development of brain metastasis16.
Herein we describe the procedures to generate brain metastasis via tail-vein injection of MDA-IBC3 cells and to evaluate the metastatic burden via stereofluorescent microscopy and luciferase imaging. This method has been used to discover key mediators of breast cancer metastasis to the brain and to test the efficacy of therapeutic interventions16,22,23. The disadvantage of this technique is that it does not recapitulate all the steps in the brain metastatic process. Nevertheless, its major advantages include robustness and reproducibility, involvement of the relevant metastasis biology of intravasation, traversing the lungs and extravasation into the brain, and its relative simplicity in terms of technique.
Protocol
The method described here has been approved by the Institutional Animal Care and Use Committee (IACUC) of the MD Anderson Cancer Center and complies with the National Institutes of Health Guidelines for the Care and Use of Laboratory Animals. The schematic workflow, with all steps included, is presented as Figure 1.
1. Cell preparation
NOTE: The MDA-IBC3 (ER–/PR–/HER2+) cell line, generated in Dr. Woodward's lab24, was stably transduced with a luciferase-green fluorescent protein (Luc-GFP) plasmid.
- Culture transduced cells in Ham's F-12 media supplemented with 10% fetal bovine serum (FBS), 1 µg/mL hydrocortisone, 5 µg/mL insulin, and 1% antibiotic-antimitotic.
- Plate MDA-IBC3-Luc-GFP cells at 37 °C and 5% CO2 in a T-75 flask until confluent. Change media every 3 days before cells are confluent enough to passage.
- Harvest cells by removing media, washing each flask with 10 mL of 1x Dulbecco's (i.e., calcium- and magnesium-free) phosphate-buffered saline (DPBS), and adding 2 mL of 0.25% trypsin-ethylenediaminetetraacetic acid (EDTA). Incubate for 3-5 min at 37 °C until cells detach.
- Add 5 mL of complete media to the flask to collect the cells and transfer the entire contents to a 15 mL centrifuge tube (optimized to 50 mL centrifuge tube depending on the total number of cells needed). Centrifuge at 290 x g for 5 min to pellet cells.
NOTE: Complete media is Ham's F-12 media supplemented with 10% fetal bovine serum (FBS), 1 µg/mL hydrocortisone, 5 µg/mL insulin, and 1% antibiotic-antimitotic. - Discard the supernatant. Then wash the cells with 10 mL of 1x DPBS. Centrifuge at 290 x g for 5 min to pellet the cells and discard the supernatant carefully. Resuspend the cells with 1 mL of fresh 1x DPBS and mix well by pipetting up and down.
- To make single-cell suspensions, filter cells through 40 µm sterile cell strainers.
- Calculate cell density by using an automated cell counter.
NOTE: To reduce errors in counting, create different cell dilutions and count them separately, and calculate the average value to determine the concentration of cells (number of cells/mL).- Collect 2 µL of cell suspension + 8 µL of 1x DPBS to make a 1:5 dilution sample.
- Collect 1 µL of cell suspension + 9 µL of 1x DPBS to make a 1:10 dilution sample.
- Add 10 µL of 0.4% trypan blue stain. Mix the sample mixture well by pipetting it up and down a few times.
- Gently pipette 10 µL of the sample into the half-moon-shaped sample loading area of the counting chamber slides. Make sure there are no bubbles inside; wait for 30 s to allow the cells to settle in the chamber before counting.
- Dilute the cells with 1x DPBS to a density of 5 x 105 or 1 x 106 cells per 100 µL. Transfer cell suspension into 1.7 mL microcentrifuge tubes for tail-vein injection. Place cells on ice until injection to maintain viability.
2. Tail vein injection
- Use 4- to 6-week-old female athymic SCID/Beige mice.
- Prepare a 30 G syringe to draw 100 µL of cell suspension. Remove all air bubbles.
- Place mouse in a rodent restrainer (diameter about 1 inch) to facilitate tail-vein injection and prevent injuries from movement during the injection process.
- Use alcohol cotton pads (made with 70% ethanol) to gently wipe the mouse's tail 3-4 times and hold for 5-10 s to make the tail vein more clearly visible.
- Insert the syringe into the tail of the mouse at an angle of 15-30°. Slowly push the cell suspension into the tail vein.
- Remove the syringe gently and use the cotton pad to hold the tail for few seconds to help stop any bleeding.
- Return the mice to their cages and check them 2-4 h after injection to ensure that no adverse effects occur.
3. Evaluation of brain metastasis burden
- Prepare diluted D-luciferin solution.
NOTE: Stock concentration is 47.6 mM (15.15 mg/mL), and the concentration for use is 1.515 mg/mL.- Add 5 mL of 1x DPBS to the D-luciferin bottle.
- Place 2.5 mL of the solution into each of two 50 mL conical tubes.
- Add another 5 mL of 1x DPBS to the D-luciferin bottle again to rinse it. Put 2.5 mL into each 50 mL conical tube.
- Place another 5 mL of 1x DPBS into the bottle and rinse it again.Repeat the rinsing process twice.
- Add 1x DPBS to each 50 mL tube to a total of 66 mL (about 33 mL per tube). There should be about 33 mL of the solution in each tube.
- Mix the tubes well and then combine both into a sterile filtration unit (150 mL PES filter 0.45 µm).
- Filter the solution and then aliquot the filtered solution into sterile amber 1.7 mL microtubes.
- Detecting brain metastases by luciferase imaging.
- Thaw D-luciferin by keeping on ice, and vortex before injection into the mice.
- Clean the area of injection with alcohol cotton pads and inject 100 µL of D-luciferin per mouse intraperitoneally by using a 0.5 mL insulin syringe, one syringe for each cage.
- After 10 min, anesthetize the mice with isoflurane (2% O2– 2.5% isoflurane) for 5 min using the veterinary vaporizer connected to the small animal induction chamber.
- Turn on the in vivo imaging system. While the mice from the first cage are under anesthesia, inject the D-luciferin into the mice in the next cage.
- Put mice into the in vivo imaging system machine and obtain ventral and dorsal images. Select an exposure time of 2 min, and in the field view choose option E (whole body). Press Acquire. Next, save the image (Figure 2).
NOTE: If the image shows saturation of luminescence, reduce the exposure time.
- Detecting brain metastases by GFP imaging.
- Brain tissue preparation.
- About 8-10 weeks post injection of cells or when the mice are moribund due to brain metastasis burden, euthanize the mice by inhalation of an isoflurane overdose followed by cervical dislocation, in accordance with protocols approved by the IACUC.
- After euthanasia with isoflurane followed by cervical dislocation, spray the mice with a 70% ethanol solution and remove the fur from the head area and ears with scissors. Next, make a cut in the cervical area of the neck (being careful to not decapitate the mouse). Cut the skull and pull it out. Next, carefully remove the brain.
- Place the collected brains into tissue cassettes.
- Transfer the cassettes to a container with cold 1x DPBS.
NOTE: Brain samples should not be kept in 1x DPBS for more than 1 h. If several brain samples are to be collected at the same time, euthanize only a few mice at a time (10 per round).
- Stereomicroscopic imaging.
- Transfer the whole brain onto a 100 cm tissue dish lid.
- Turn on the stereomicroscope and the UV light, at position 3 with lens 0.5x, to allow visualization of the whole brain as shown in Figure 3A (red square).
- Press Live view (Figure 3A, green square).
- Focus the view while the brain is in the ventral position.
- Select GFP (if cells are GFP-labeled) or TXRED (if cells are RFP-labeled) (Figure 3A, yellow square) in the software, select the proper filter on the microscope, and take a picture.
NOTE: Keep the SOLA light source setting at about 30%; if the GFP is too bright, reduce until the proper signal is observed. - Without moving the sample, turn on the bright light and select BF (Figure 3A, yellow square). Take a picture.
- Repeat the previous steps with the brain in the dorsal position.
NOTE: Depending on the size, the same GFP positive brain metastasis lesion can appear in both ventral and dorsal positions. In such a case, avoid duplicate quantification of the same lesion. Save the images with a TIFF extension (which keeps all the information in the picture file). - Save the images with a TIFF extension (which keeps all the information in the picture file).
- Repeat steps for all samples.
- Convert the TIFF images into JPEG so that the files can be opened with any computer that does not have the associated software installed (File | Import/Export | convert files).
- To merge the fluorescent image with the bright field image, open both images and go to File | Merge channels. Select the proper components, green for GFP and brightfield for BF, and press Ok. Save the merged image.
- To quantify brain tumor area, use the fluorescent image. Select Measure | Manual Measurement | Area. Select automatic selection (Figure 3B, green square), and move the arrow to the GFP-positive area and click to automatically create a selection. Click again to confirm the selection and then all measurements will show (Figure 3B, red square). If more than one GFP-positive area is present, repeat the procedure.
- After brain images are obtained, proceed to routine tissue fixation protocols using 10% neutral buffered formalin.
- Once the brains are fixed, proceed to standard histological sectioning followed by hematoxylin and eosin staining to confirm the presence of brain metastasis and immunohistochemical staining to detect selected markers.
NOTE: Immunocytochemistry was performed at the Pathology Core Laboratory at UT MD Anderson Cancer Center that has standardized protocol for immunohistochemical staining of known markers.
- Once the brains are fixed, proceed to standard histological sectioning followed by hematoxylin and eosin staining to confirm the presence of brain metastasis and immunohistochemical staining to detect selected markers.
- Brain tissue preparation.
Representative Results
With the rationale that labeled cells facilitate monitoring and visualization of brain metastasis in preclinical mouse models, we tagged MDA-IBC3 cells with Luc and with GFP to monitor brain metastases and quantify the metastatic burden by using bioluminescence imaging and fluorescent stereomicroscopy. Injection of the labeled MDA-IBC3 cells into the tail veins of immunocompromised SCID/Beige mice resulted in high percentages of mice developing brain metastasis (i.e., 66.7% to 100 %)16,23,25. Brain metastatic lesions could be detected as early as 8 weeks after injection by luciferase imaging (Figure 2) or stereofluorescent microscopy (Figure 4). GFP imaging allows us to detect, count, and calculate the area of each metastatic lesion. After imaging, portions of the brain metastases are formalin-fixed and processed for hematoxylin and eosin staining to validate the presence of brain metastasis lesions (Figure 5A) and for immunohistochemical staining to detect specific protein markers (Figure 5B,C).
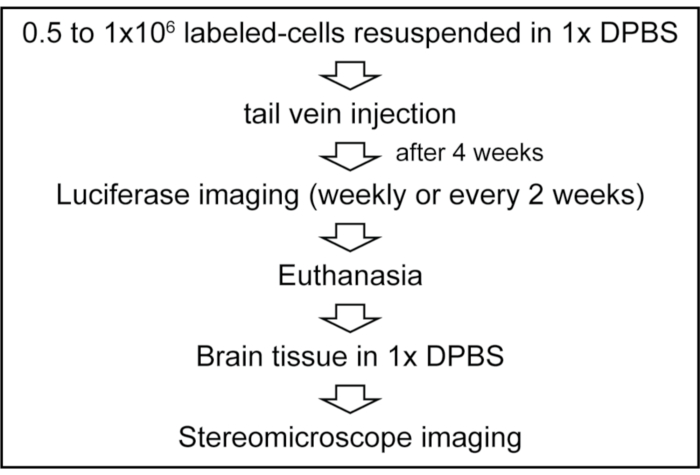
Figure 1: Schematic workflow for generating brain metastasis via tail-vein injection. Please click here to view a larger version of this figure.
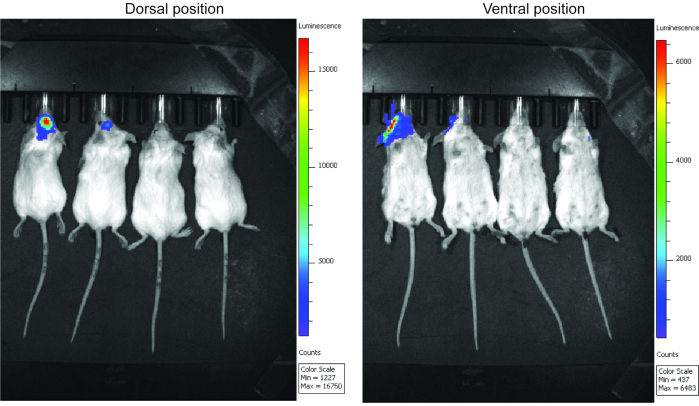
Figure 2: Luciferase images of mice in dorsal and ventral positions. Please click here to view a larger version of this figure.
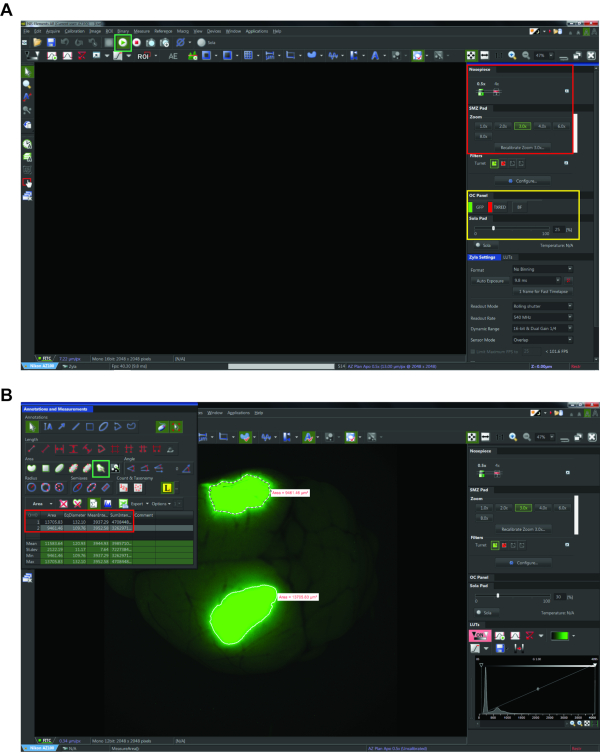
Figure 3: Screenshots of imaging software used for stereomicroscopy. (A) Steps showing how to obtain images. The green square on the left shows the live view button; the red square on the right shows the position of the microscope for the nosepiece lens and zoom position; and the yellow square highlights the filter selection. (B) Screenshot of the steps involved in measuring tumor burden. The green square at upper left shows the auto selection mode for area calculation; the red square beneath it shows the area values and other measurements after the brain metastasis lesion was selected. Please click here to view a larger version of this figure.
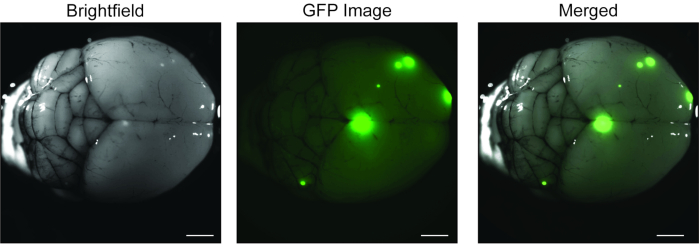
Figure 4: Stereoscopic images of mouse brains with metastases from tail-vein injection of the MDA-IBC3 cell line. The brightfield picture on the left is merged with the GFP image (middle) and then merged (right). Scale bar = 100 µm. Please click here to view a larger version of this figure.
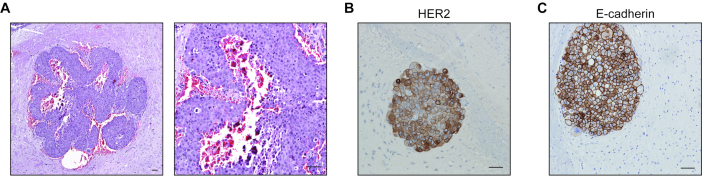
Figure 5: Slides showing stained images of MDA-IBC3-derived brain metastases in mice. (A) Hematoxylin and eosin stains provide histologic confirmation of brain metastasis. Immunostaining of the MDA-IBC3-derived brain metastatic tumors show positive staining for HER2 (B) and E-cadherin (C). Scale bar = 100 µm. Please click here to view a larger version of this figure.
Discussion
The protocol includes several critical steps. Cells should be kept on ice for no longer than 1 hour to maintain viability. Alcohol cotton pads should be used to wipe the tails of the mice before injection, with care taken to not wipe too hard or too often to avoid damaging the tail skin. Ensure that no air bubbles are present in the cell suspension, to prevent mice from dying from blood vessel emboli. Maintain the angle of injection at 45° or less to avoid piercing the blood vessel in the tails and insert at least 1/3 of the needle into the tail-vein to ensure successful injection of all cells. The total volume of injected cells can be adjusted according to the weight of the mice, but the total number of cells should be kept as similar as possible. In this protocol, the SCID / Beige mice were all 4 to 6 weeks old and weighed between 15 and 20 g. For mice that weigh less than 15 g, the injection volume could be adjusted to less than 100 µL; otherwise, 100 µL is injected. After its removal from the skull, the whole brain must be kept in 1x DPBS for no longer than 1 hour before imaging by stereoscopic microscopy to prevent signal reduction and tissue degeneration. For immunofluorescence imaging, brain tissues should not be placed in formalin, because it generates endogenous autofluorescence that hinders the acquisition of high-quality images. We have noted that luciferase imaging does not always reveal brain metastases, especially very small lesions; however, GFP imaging by stereomicroscopy can visualize all lesions. Moreover, GFP imaging can show more than 1 lesion, whereas luciferase imaging does not.
The proposed procedures can be modified slightly according to user preferences. First, the number of injected cells and the duration of metastasis formation could be adjusted for different studies. Second, the tail vein of the mice could be visualized more clearly by using warm water to dilate the vein or UV light to illuminate the veins. Finally, the size of the needle in the syringe can be either 30 G or 28 G.
The advantages and limitations of existing mouse models of brain metastasis has been reviewed elsewhere3 .The brain metastasis model we described here does have its limitations and strengths. One limitation is that it does not recapitulate all the steps of the brain metastatic process and does not allow interrogation of the initial stages of the metastatic process, i.e., the dissemination of primary breast cancer cells into the circulation. Also, this model cannot be used to study the interactions between tumor cells and the host immune microenvironment during the process of brain metastasis or to evaluate immunotherapeutic applications. However, this model has several advantages over other brain metastasis models. First, unlike spontaneous models in which only a small fraction of the mice develop brain metastases at variable intervals, our model offers the advantage of consistently leading to metastasis to the brain, typically in more than 70% of mice. Second, tail-vein injection allows the dissemination of cells primarily to the lung with subsequent spread to the brain, whereas inoculation via the intracarotid artery allows cells to disseminate directly to the brain; intracardiac injections allow systemic distribution of the cancer cells to the brain as well as to extracranial sites such as the lung and bone. Thus, our model recapitulates the brain metastatic colonization step better than the commonly used intracardiac or intracarotid injection models because the cells traverse the lung capillary beds and survive in the circulation before generating brain lesions. Finally, injection of breast cancer cells via the tail vein is technically less challenging than intracarotid or intracardiac injection.
Divulgazioni
The authors have nothing to disclose.
Acknowledgements
We thank Christine F. Wogan, MS, ELS, of MD Anderson’s Division of Radiation Oncology for scientific editing of the manuscript, and Carol M. Johnston from MD Anderson’s Division of Surgery Histology Core for help with hematoxylin and eosin staining. We are thankful to the Veterinary Medicine and Surgery Core at MD Anderson for their support for the animal studies. This work was supported by the following grants: Susan G. Komen Career Catalyst Research grant (CCR16377813 to BGD), American Cancer Society Research Scholar grant (RSG-19–126–01 to BGD), and the State of Texas Rare and Aggressive Breast Cancer Research Program. Also supported in part by Cancer Center Support (Core) Grant P30 CA016672 from the National Cancer Institute, National Institutes of Health, to The University of Texas MD Anderson Cancer Center.
Materials
| Cell Culture | |||
| 1000 µL pipette tip filtered | Genesee Scientific | 23430 | |
| 10 mL Serological Pipets | Genesee Scientific | 12-112 | |
| Antibiotic-antimycotic | Thermo Fisher Scientific | 15240062 | 1% |
| Centrifuge tubes 15 mL bulk | Genesee Scientific | 28103 | |
| Corning 500 mL Hams F-12 Medium [+] L-glutamine | GIBICO Inc. USA | MT10080CV | |
| Countess II Automated Cell Counter (Invitrogen) | Thermo Fisher Scientific | AMQAX1000 | |
| 1x DPBS | Thermo Fisher Scientific | 21-031-CV | |
| Eppendorf centufuge 5810R | Eppendorf | ||
| Fetal bovine serum (FBS) | GIBICO Inc. USA | 16000044 | 10% |
| Fisherbrand Sterile Cell Strainers (40 μm) | Thermo Fisher Scientific | 22-363-547 | |
| Hydrocortisone | Sigma-Aldrich | H0888 | 1 µg/mL |
| Insulin | Thermo Fisher Scientific | 12585014 | 5 µg/mL |
| Invitrogen Countess Cell Counting Chamber Slides | Thermo Fisher Scientific | C10228 | |
| MDA-IBC3 cell lines | MD Anderson Cancer Center | Generated by Dr. Woodward's lab24 | |
| Luciferase–green fluorescent protein (Luc–GFP) plasmid | System Biosciences | BLIV713PA-1 | |
| microtubes clear sterile 1.7 mL | Genesee Scientific | 24282S | |
| Olympus 10 µL Reach Barrier Tip, Low Binding, Racked, Sterile | Genesee Scientific | 23-401C | |
| TC Treated Flasks (T75), 250mL, Vent | Genesee Scientific | 25-209 | |
| Trypan Blue Stain (0.4%) for use with the Countess Automated Cell Counter | Thermo Fisher Scientific | T10282 | |
| Trypsin-EDTA (0.25%), phenol red | Thermo Fisher Scientific | 25200114 | |
| Tail vein injection | |||
| C.B-17/IcrHsd-Prkdc scid Lyst bg-J – SCID/Beige | Envigo | SCID/beige mice | |
| BD Insulin Syringe with the BD Ultra-Fine Needle 0.5mL 30Gx1/2" (12.7mm) | BD | 328466 | |
| Plas Labs Broome-Style Rodent Restrainers | Plas Labs 551BSRR | 01-288-32A | Order fromThermo Fisher Scientific |
| Volu SolSupplier Diversity Partner Ethanol 95% SDA (190 Proof) | Thermo Fisher Scientific | 50420872 | 70 % used |
| Imaging | |||
| BD Lo-Dose U-100 Insulin Syringes | BD | 329461 | |
| Disposable PES Filter Units 0.45 µm | Fisherbrand | FB12566501 | filter system to sterilize the D-luciferin |
| D-Luciferin | Biosynth | L8220-1g | stock concentration = 47.6 mM (15.15 mg/mL); use concentration = 1.515 mg/mL |
| 1.7 mL microtube amber | Genesee Scientific | 24-282AM | |
| Isoflurane | Patterson Veterinary | NDC-14043-704-06 | Liquid anesthetic for use in anesthetic vaporizer |
| IVIS 200 | PerkinElmer | machine for luciferase imaging, up to 5 mice imaging at the same time, with anesthesia machine | |
| Plastic Containers with Lids | Fisherbrand | 02-544-127 | |
| Tissue Cassettes | Thermo Scientific | 1000957 | |
| Webcol Alcohol Prep | Covidien | 6818 | |
| Stereomicroscope Imaging | |||
| Stereomicroscope AZ100 | Nikon | model AZ-STGE | software NIS-ELEMENT |
| Formalin 10% | Fisher Chemical | SF100-4 | |
| TC treated dishes 100×20 mm | Genesee Scientific | 25202 |
Riferimenti
- Achrol, A. S., et al. Brain metastases. Nature Reviews Disease Primers. 5 (1), 5 (2019).
- Nayak, L., Lee, E. Q., Wen, P. Y. Epidemiology of brain metastases. Current Oncology Report. 14 (1), 48-54 (2012).
- Lowery, F. J., Yu, D. Brain metastasis: Unique challenges and open opportunities. Biochimica et Biophysica Acta Review Cancer. 1867 (1), 49-57 (2017).
- Brufsky, A. M., et al. Central nervous system metastases in patients with HER2-positive metastatic breast cancer: incidence, treatment, and survival in patients from registHER. Clinical Cancer Research. 17 (14), 4834-4843 (2011).
- Valiente, M., et al. The evolving landscape of brain metastasis. Trends in Cancer. 4 (3), 176-196 (2018).
- Bos, P. D., et al. Genes that mediate breast cancer metastasis to the brain. Nature. 459 (7249), 1005-1009 (2009).
- Woditschka, S., et al. DNA double-strand break repair genes and oxidative damage in brain metastasis of breast cancer. Journal of the National Cancer Institute. 106 (7), (2014).
- Palmieri, D., et al. Vorinostat inhibits brain metastatic colonization in a model of triple-negative breast cancer and induces DNA double-strand breaks. Clinical Cancer Research. 15 (19), 6148-6157 (2009).
- Kim, S. J., et al. Astrocytes upregulate survival genes in tumor cells and induce protection from chemotherapy. Neoplasia. 13 (3), 286-298 (2011).
- Zhang, S., et al. SRC family kinases as novel therapeutic targets to treat breast cancer brain metastases. Ricerca sul cancro. 73 (18), 5764-5774 (2013).
- Valiente, M., et al. Serpins promote cancer cell survival and vascular co-option in brain metastasis. Cell. 156 (5), 1002-1016 (2014).
- Gril, B., et al. Effect of lapatinib on the outgrowth of metastatic breast cancer cells to the brain. Journal of the National Cancer Institute. 100 (15), 1092-1103 (2008).
- Gril, B., et al. Pazopanib reveals a role for tumor cell B-Raf in the prevention of HER2+ breast cancer brain metastasis. Clinical Cancer Research. 17 (1), 142-153 (2011).
- Palmieri, D., et al. Profound prevention of experimental brain metastases of breast cancer by temozolomide in an MGMT-dependent manner. Clinical Cancer Research. 20 (10), 2727-2739 (2014).
- Priego, N., et al. STAT3 labels a subpopulation of reactive astrocytes required for brain metastasis. Nature Medicine. 24 (7), 1024-1035 (2018).
- Debeb, B. G., et al. miR-141-mediated regulation of brain metastasis from breast cancer. Journal of the National Cancer Institute. 108 (8), (2016).
- Chang, S., Parker, S. L., Pham, T., Buzdar, A. U., Hursting, S. D. Inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program of the National Cancer Institute, 1975-1992. Cancer. 82 (12), 2366-2372 (1998).
- Hance, K. W., Anderson, W. F., Devesa, S. S., Young, H. A., Levine, P. H. Trends in inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program at the National Cancer Institute. Journal of National Cancer Institute. 97 (13), 966-975 (2005).
- Dirix, L. Y., Van Dam, P., Prove, A., Vermeulen, P. B. Inflammatory breast cancer: Current understanding. Current Opinion in Oncology. 18 (6), 563-571 (2006).
- Wang, Z., et al. Pattern of distant metastases in inflammatory breast cancer – A large-cohort retrospective study. Journal of Cancer. 11 (2), 292-300 (2020).
- Uemura, M. I., et al. Development of CNS metastases and survival in patients with inflammatory breast cancer. Cancer. 124 (11), 2299-2305 (2018).
- Smith, D. L., Debeb, B. G., Thames, H. D., Woodward, W. A. Computational modeling of micrometastatic breast cancer radiation dose response. International Journal of Radiation Oncology, Biology, Physics. 96 (1), 179-187 (2016).
- Fukumura, K., et al. Multi-omic molecular profiling reveals potentially targetable abnormalities shared across multiple histologies of brain metastasis. Acta Neuropathol. , (2021).
- Klopp, A. H., et al. Mesenchymal stem cells promote mammosphere formation and decrease E-cadherin in normal and malignant breast cells. PLoS One. 5 (8), 12180 (2010).
- Villodre, E. S., et al. Abstract P3-01-10: Ndrg1-egfr axis in inflammatory breast cancer tumorigenesis and brain metastasis. Ricerca sul cancro. 80 (4), 10 (2020).
