NOTE: All experiments were performed in strict accordance with institutional guidelines for the care and use of animals in research. The protocol was approved by the Administration of the Republic of Slovenia for Food Safety, Veterinary Sector and Plant Protection (permit number: 34401-35-2018/2).
1. Preparation of pancreatic tissue slices
NOTE: The preparation of acute mouse pancreas tissue slices for calcium imaging using CLSM requires a number of instruments, different solutions, and proceeds in a series of critical steps that are schematically presented in Figure 1 and described in detail below.
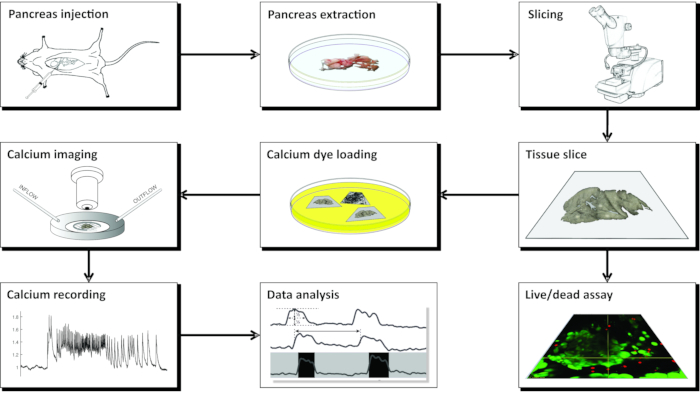
Figure 1: Workflow diagram. Schematic representation of all steps in the process of pancreatic tissue slice preparation, beginning with the injection of agarose into the common bile duct, followed by extraction of the pancreas and slicing. The prepared slices can be used for assessing the viability of the tissue with a Live/Dead kit or stained with a calcium sensor. Once stained, they are ready for imaging. Recordings obtained from the imaging process are then used for data analysis. Please click here to view a larger version of this figure.
- Preparation of solutions
NOTE: All solutions should be prepared in advance and can be stored in the refrigerator at 4-8 °C for up to one month. For the preparation and storage of tissue slices, approximately 0.5 L of extracellular solution (ECS) with 6 mM glucose and 0.3 L of 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) buffer is needed. For 1 day of calcium imaging with the perifusion system set at 1-2 mL/min flow rate, approximately 0.5 L of ECS is needed.- Extracellular solution with 6 mM glucose
- Prepare 1 L of ECS containing 125 mM NaCl, 26 mM NaHCO3, 6 mM glucose, 6 mM lactic acid, 3 mM myo-inositol, 2.5 mM KCl, 2 mM Na pyruvate, 2 mM CaCl2, 1.25 mM NaH2PO4, 1 mM MgCl2, and 0.5 mM ascorbic acid. Mix thoroughly until all ingredients completely dissolve. Take 50 μL of ECS into an 0.5 mL microcentrifuge tube, place it onto the osmometer according to the manufacturer's instructions, and check the osmolarity.
NOTE: The osmolarity should be 300-320 mOsm. For stimulation of beta cells, use solutions with higher glucose concentrations. To ensure physiological pH value of 7.4 during slicing and experiments, constantly bubble the ECS with carbogen (i.e., a gas mixture of 95% O2 and 5% CO2) at barometric pressure. A simple bubbling system can be set up by attaching one end of a 5 mm silicon tubing to the source of carbogen (i.e., a pressurized gas cylinder) and the other end of the tubing placed directly into the bottle containing ECS. - Alternatively, prepare a 10x stock containing 1250 mM NaCl, 260 mM NaHCO3, 30 mM myo-inositol, 25 mM KCl, 20 mM Na pyruvate, 12.5 mM NaH2PO4, and 5 mM ascorbic acid. When the ECS containing 6 mM glucose is needed, mix 100 mL of the stock with 2 mL of 1 M CaCl2, 1 mL of 1 M MgCl2, 0.455 mL of 13.2 M lactic acid, and 1.08 g of glucose, and fill with double-distilled water up to 1 L. If needed, use different amounts of glucose to obtain other glucose concentrations.
- Prepare 1 L of ECS containing 125 mM NaCl, 26 mM NaHCO3, 6 mM glucose, 6 mM lactic acid, 3 mM myo-inositol, 2.5 mM KCl, 2 mM Na pyruvate, 2 mM CaCl2, 1.25 mM NaH2PO4, 1 mM MgCl2, and 0.5 mM ascorbic acid. Mix thoroughly until all ingredients completely dissolve. Take 50 μL of ECS into an 0.5 mL microcentrifuge tube, place it onto the osmometer according to the manufacturer's instructions, and check the osmolarity.
- HEPES buffer with 6 mM glucose
- Prepare 0.5 L of HEPES-buffered solution (HBS) containing 150 mM NaCl, 10 mM HEPES, 6 mM glucose, 5 mM KCl, 2 mM CaCl2, and 1 mM MgCl2; titrate to pH = 7.4 with 1 M NaOH.
NOTE: If carbogen is not available, this buffer can be used for all steps instead of ECS.
- Prepare 0.5 L of HEPES-buffered solution (HBS) containing 150 mM NaCl, 10 mM HEPES, 6 mM glucose, 5 mM KCl, 2 mM CaCl2, and 1 mM MgCl2; titrate to pH = 7.4 with 1 M NaOH.
- Agarose (1.9% w/w)
- Prewarm a water bath to 40 °C.
- Add 0.475 g of low-melting-point agarose and 25 mL of ECS containing 6 mM glucose to an Erlenmeyer flask, and place the flask in a microwave oven at maximum power for a few seconds until it starts to boil. Take the flask out of the oven and swirl it a few times, until the agarose dissolves completely. Transfer the flask with the liquid agarose to the prewarmed water bath at 40 °C to cool the agarose to the desired temperature and to keep it liquid until injection. Secure the flask with a stabilizing lead ring.
NOTE: The agarose can be prepared in advance and kept in the refrigerator. Before use, warm the agarose in the microwave oven until it liquefies, and transfer the Erlenmeyer flask into a water bath prewarmed to 40 °C. The agarose can be re-used up to 5x. If re-used beyond 5x, it will become dense and harder to inject.
- Extracellular solution with 6 mM glucose
- Injection of pancreas with agarose
NOTE: Sections 1.2 and 1.3 explain the preparation of tissue slices that can be used for different experimental purposes such as calcium imaging, electrophysiology, immunohistochemistry, secretion studies, and structural/microanatomical studies.- Fill a 5 mL syringe with the liquid agarose from the Erlenmeyer flask in the water bath from step 1.1.3.2, remove any bubbles, and mount a 30 G needle. Protect the needle with a cap, and keep the filled syringe back in the water bath with the needle facing downward and the entire volume of agarose below the water surface. Secure the syringe with a stabilizing lead ring in such way that the ring presses the syringe against the wall of the water bath.
NOTE: Be careful not to push any agarose into the needle as it will harden quickly and block the needle. If the room temperature is low, and if the injection is performed by a less experienced person, increase the temperature of the water bath up to 42 °C to gain some additional time for injection. - Fill an ice bucket with ice, and place the bottle containing ECS in it. Bubble the ECS constantly at 1.5 mL/min with carbogen at barometric pressure and room temperature to ensure oxygenation and a pH of 7.4.
- Sacrifice a mouse by administering a high concentration of CO2 followed by cervical dislocation. Make all efforts to minimize animal suffering.
- Working under a stereomicroscope, access the abdomen via laparotomy (Figure 2A). Gently flip the gut to the left side of the mouse (from the anatomical perspective of the mouse) to expose the common bile duct. Use forceps to slightly lift the duodenal part, and find the major duodenal papilla-papilla of Vater. Clamp the common bile duct at the duodenal papilla using a hemostat (Figure 2B,C) to prevent leakage of agarose from the duct into the duodenum.
NOTE: To prevent agarose leakage into the duodenum and further up and down in the gastrointestinal tract, place the hemostat in such a way that it also clamps the duodenum both proximally and distally from the papilla. It is best to use a curved hemostat for this purpose. - With small sharp forceps, reach under the common bile duct, and break the membrane that attaches the duct to the pancreatic tissue. For better visual control and easier injection, clear as much fat and connective tissue from the duct as possible.
- Place the duct perpendicularly onto large forceps (Figure 2D), and inject the prepared liquid agarose into the proximal part of the common bile duct (Figure 2D). Be sure to squeeze the syringe hard as the agarose is viscous. Keep filling the pancreas until it becomes whitish and slightly distended or for at least 20-30 s.
NOTE: This is the most critical step in slice preparation. If there are any kinks in the ductal tree of the pancreas, gently elevate or pull the pancreas away from the syringe to level them out. Do not decide when to stop injection based on the volume injected from the syringe as the backflow at the point of injection and forward leakage into the duodenum are typically much higher than the volume injected into the ductal tree of the pancreas. Importantly, successful injections can be performed with practically unnoticeable changes in syringe volume. - Remove the syringe, and slowly pour 20 mL of the bubbled ice-cold ECS at 0-4 °C from the bottle onto the pancreas to cool the tissue and harden the agarose.
- Gently extract the pancreas using forceps and fine tough-cut scissors. Place the extracted pancreas into a 100 mm Petri dish containing ~40 mL of ice-cold ECS, and gently move it around to wash it. Transfer the pancreas into a fresh 100 mm Petri dish containing ~40 mL of ice-cold ECS.
- From the well-injected part of the pancreas, which appears whitish (Figure 3A), cut up to 6 blocks of tissue, 0.1-0.2 cm3 in size, using forceps and tough-cut scissors. Clear them of any connective and fatty tissue.
- Fill a 35 mm non-sticky bottom-Petri dish with approximately 5 mL of liquid agarose at 40 °C, transfer the tissue blocks into it, and immediately put the Petri dish on ice to cool it down and harden the agarose.
NOTE: The way the blocks of pancreas are trapped in agarose determines the way they are cut during slicing. Experienced experimentalists can try and fine-tune the position of the blocks during the few moments before the agarose hardens when placed on ice. - After the agarose with the tissue blocks hardens, turn the Petri dish upside down onto a flat smooth surface such as the lid of a 100 mm Petri dish, and remove the agarose by gently cutting with one half of a razor blade into the margin between the lateral wall of the Petri dish and the agarose. With a razor blade, cut individual agarose cubes, each containing one tissue block, taking care that each tissue block is surrounded by agarose. Glue the agarose blocks onto the sample plate of the vibratome with cyanoacrylate glue (Figure 3B).
- Fill a 5 mL syringe with the liquid agarose from the Erlenmeyer flask in the water bath from step 1.1.3.2, remove any bubbles, and mount a 30 G needle. Protect the needle with a cap, and keep the filled syringe back in the water bath with the needle facing downward and the entire volume of agarose below the water surface. Secure the syringe with a stabilizing lead ring in such way that the ring presses the syringe against the wall of the water bath.
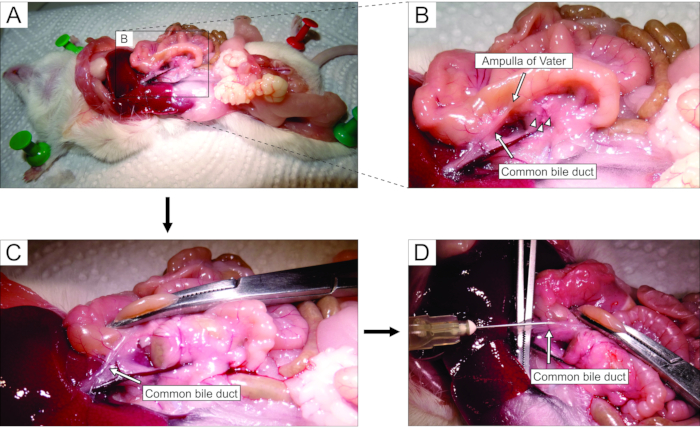
Figure 2: Injection of agarose into the common bile duct. (A) Open the abdominal cavity, and expose the organs in the peritoneal cavity. (B) The magnified part of the area enclosed by the rectangle in panel A. The white spot on the duodenum (indicated by the arrow) indicates the ampulla of Vater. Islets of Langerhans are denoted by arrowheads. (C) Clamp the ampulla of Vater by a curved hemostat, and raise it slightly to expose and gently stretch the common bile duct (arrow). (D) Cannulation of the common bile duct and the injection of 1.9% agarose solution using a 5 mL syringe and a 30 G needle. Please click here to view a larger version of this figure.
- Slicing
- Fill the cutting chamber of the vibratome with ~0.15 L of ice-cold ECS, and bubble constantly with carbogen. Surround the cutting chamber with ice, and add 2 ice cubes (~10 mL each) made of ECS with 6 mM glucose into the cutting chamber. Mount the razor blade for cutting onto the vibratome, and screw-fix the sample plate with agarose blocks into its place.
- Set the slicer to cut agarose blocks at 0.05 to 1 mm/s and 70 Hz into 140 µm-thick slices with a surface area of 20-100 mm2. For slicer settings, follow the manufacturer's instructions.
- Immediately after each cutting step, pause the slicer, gently collect the slices with a fine paint brush, and transfer them into a 100 mm Petri dish filled with 40 mL of HEPES buffer with 6 mM glucose at room temperature (Figure 3C).
NOTE: The slices can be kept in HEPES buffer at room temperature for at least 12 h, and the buffer should be exchanged every 2 h.
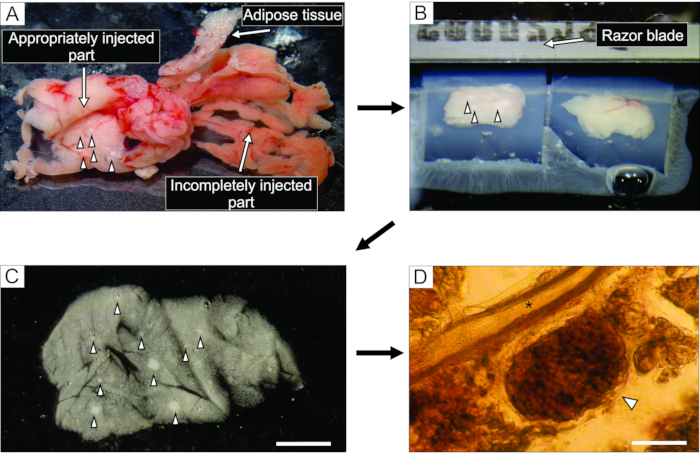
Figure 3: Pancreas tissue preparation and slicing. (A) The extracted mouse pancreas after agarose injection. White tissue on the left indicates a well-injected part (duodenal part), while the more reddish part on the right shows the insufficiently injected part of the pancreas (splenic part). (B) Vibratome slicing of two blocks of pancreas tissue embedded in agarose. (C) Acute pancreatic tissue slice with islets of Langerhans indicated by arrowheads. Scale bar = 3000 µm. (D) Acute pancreatic tissue slice under the light microscope with the islet of Langerhans indicated by an arrowhead, asterisk indicates a pancreatic duct. Scale bar = 100 µm. Please click here to view a larger version of this figure.
2. Live/dead assay using LIVE/DEAD Viability/Cytotoxicity Kit for mammalian cells
NOTE: For some experiments, it is useful to check the viability of cells in the slices (Figure 4) by the live/dead assay as follows.
- Follow the manufacturer's instructions to thaw vials with reagents of the LIVE/DEAD Viability/Cytotoxicity Kit, and prepare working solutions of calcein AM just before use. Use the solutions within one day.
- In a 15 mL centrifuge tube, mix 5 µL of 4 mM calcein AM (Component A), 20 µL of 2 mM ethidium homodimer-1 (EthD-1, Component B), and 10 mL of Dulbecco's Phosphate-buffered Saline (D-PBS) to prepare a working solution containing approximately 2 µM calcein AM and 4 µM EthD-1. Vortex thoroughly.
- Using a fine paint brush, gently transfer the tissue slices into a 3 mL Petri dish with fresh HEPES buffer to dilute serum esterase activity. Remove the HEPES buffer, and cover the slices with 100-200 µL (or more if necessary) of the working solution from step 2.2.
- Incubate the slices for 30-45 min at room temperature in a closed Petri dish. Image the tissue slices using excitation/emission filters as recommended by the manufacturer.
3. Calcium dye loading
NOTE: Fluorescent dyes should be shielded from light exposure during the whole process of preparation and loading of the dye, as well as during handling of the stained tissue slices. Tin foil can be used to cover tubes or Petri dishes containing the calcium dye.
- Dye preparation
- Dissolve the contents of one vial (50 µg) of the cell permeable Ca2+ indicator dye (excitation/emission 495/523 nm; see the Table of Materials), 7.5 µL of dimethylsulfoxide (DMSO), and 2.5 µL of the polaxamer (20% solution in DMSO; Table of Materials) in 6.667 mL of HBS containing 6 mM glucose in a 15 mL screw cap tube.
NOTE: This final solution contains 6 µM of the Ca2+ indicator dye, 0.11% DMSO, and 0.037% polaxamer. - Aspirate and expel the solution in the screw cap tube repeatedly with a pipette for 20 s; submerge the tube in an ultrasonic bath chamber for 30 s, and vortex for 30 s to improve solubilization. Aliquot 3.333 mL of the final Ca2+ indicator dye solution prepared in step 3.1.1 into 5 mL Petri dishes.
- Dissolve the contents of one vial (50 µg) of the cell permeable Ca2+ indicator dye (excitation/emission 495/523 nm; see the Table of Materials), 7.5 µL of dimethylsulfoxide (DMSO), and 2.5 µL of the polaxamer (20% solution in DMSO; Table of Materials) in 6.667 mL of HBS containing 6 mM glucose in a 15 mL screw cap tube.
- Dye loading
- Transfer the prepared tissue slices from the 60 mL Petri dish with HBS into 5 mL Petri dishes filled with the dye solution by gently lifting each tissue slice using a thin, soft paint brush and placing it in the dye solution. Incubate up to 10 tissue slices per Petri dish.
- Place the slice-loaded Petri dish on an orbital shaker at room temperature set to orbital motion at 40 turns per minute for 50 min. Incubate the slices in the dye solution exposed to ambient air at room temperature, but shielded from light by covering the Petri dish with tin foil.
- Storing of slices
- Transfer the stained tissue slices from the 5 mL Petri dish into a 60 mL Petri dish filled with dye-free HBS by gently lifting them using a fine, soft paint brush. Store up to 20 slices per Petri dish.
NOTE: Use the tissue slices for imaging at this point. The tissue slices will retain the Ca2+ indicator dye for several hours. The survival of slices and retention of the dye can be improved by placing the Petri dish in an insulated container, surrounded by ice. This is especially important if the dye-loaded slices are to be transported. Additionally, exchange the HBS every 2 h.
- Transfer the stained tissue slices from the 5 mL Petri dish into a 60 mL Petri dish filled with dye-free HBS by gently lifting them using a fine, soft paint brush. Store up to 20 slices per Petri dish.
4. Calcium imaging
- Setup of the confocal microscope
- Choose an appropriate objective magnification depending on the interest of the study. Select 20x and 25x (numerical aperture [NA] 0.77-1.00) for visualizing a whole islet, several acini simultaneously, or larger ducts. Select higher magnifications to study intracellular dynamics.
- Choose the acquisition mode for time-lapse imaging (e.g., time-lapse, xyt, or similar mode). Set the pinhole to 100-200 µm.
- Set the light path for green fluorophores: excitation at 488 nm, and collection of emission at 500-700 nm. Preferably select detectors with a high quantum efficiency (e.g., gallium arsenide phosphide) over photomultiplier detectors.
- Setup of the recording chamber and the perifusion system
- Mount the recording chamber on the temperature-controlled stage of the microscope and the perifusion system (either gravity-fed or peristaltic-pump-based setup, volume 1 mL). Position the inlet and the outlet on the far edges of the recording chamber to avoid meandering of the perfusate within the chamber, and set the inflow and the outflow to equal values (1-2 mL/min). Avoid drifting of the liquid meniscus height and droplets in the perifusate.
- Set the temperature control of the perifusion system to 37 °C.Initiate the perifusion with the non-stimulatory solution, and prepare the stimulating solutions. Change the solutions via motorized valves or by manually switching the solutions that feed the perifusion system.
- Record calcium dynamics
- Transfer a single tissue slice into the recording chamber. Immobilize the tissue slice with a U-shaped platinum weight with taut nylon mesh (e.g., from nylon stockings). Avoid positioning nylon threads over the structure of interest.
- Locate an islet/acinus/duct using the brightfield option. Run live imaging to position the studied structures into the field of view, and set up the imaging parameters. Optimize the signal-to-noise ratio by adjusting the laser power, detector amplification, and line averaging/binning to allow visualization of the cells while keeping the laser power minimal.
- Adjust the focal plane of the recording to ~15 µm below the cut surface (Figure 5) to avoid recording from potentially damaged cells at the cut surface.
- Acquire images. Set the sampling frequency to 1-2 Hz to detect individual oscillations initially, and use a resonant scanner capable of fast line averaging (8-20) at a higher acquisition rate (>10 Hz) to record intracellular Ca2+ ([Ca2+]IC) activity. Allow an interval (e.g., 30% of the total sampling time) between consecutive point illuminations to prevent phototoxicity. Record a high-resolution image (e.g., 1024 x 1024 pixels, line averaging > 50) before the time series acquisition (see section 5).
NOTE: The sampling frequency of 1-2 Hz is below the Nyquist criterion for acquisition frequency for most cells, and the shape of the signal will be undersampled by default. - Refer to an online chart, if available in the imaging software, to obtain instant feedback on the preparation response, over-illumination, photobleaching, and mechanical drift. In case of a high rate of bleaching during acquisition, stop the recording and decrease laser power while increasing the detector gain to maintain the signal-to-noise ratio. In the case of mechanical drift, check for tension between tubing/cables and the microscope stage as well as liquid leakage or changes of the volume in the recording chamber. Optionally, attempt to correct the drift during acquisition manually; however, note that this will inherently yield limited results.
NOTE: Endocrine cells are highly heterogeneous at near-threshold concentrations. A sufficient length of stimulation is needed to detect the range of activation/deactivation delays in individual cells. This is especially important for accurate detection of off-responses following highly stimulatory protocols. - Use calcium imaging to functionally discriminate between endo- and exocrine cells (Figure 6). To record transient activity during activation and deactivation, apply stimuli without stopping the recording.
- Save the data after the end of experimentation (consider using an auto-save function). Allow a cooling period before switching off the laser power so as not to damage the lasers during the shutdown procedure.
5. Analysis of data
- Visually inspect the recording qualitatively by replaying the time-lapse video. Check for cell drifts from the field of view or the optical plane. If a drift within the optical plane has occurred, employ the drift correction plugin in ImageJ.
- Select regions of interest (ROIs) using microscope software or third-party software. Use the high-resolution image, maximal projection, or frame average as the reference to select ROIs. Replay the time-lapse imaging to visualize responding cells that are not visible in reference images. Position the ROIs such that the selected area of a ROI does not overlap with neighboring cells to avoid signal crosstalk between ROIs.
- Export the time series data as ROI average value per frame. Export ROI coordinates.
- Correct the time series data for bleaching (Figure 7A) by employing a combination of an exponential and linear fit, as described by
 (1)
(1)
where x(t) denotes the fluorescence signal at a time point t; xcorr(t) the corrected signal at the corresponding time points; and a, b, and c the parameters of the fit calculated as the least sum of squares between the corr(t) and x(t). - Analyze the activation and deactivation phase of the response (Figure 7B). Calculate the first derivative of the time series data, and determine the zenith and the nadir of the derivative corresponding to the activation and deactivation, respectively. Alternatively, manually select the start of the phasic increase. Save and export the activation/deactivation times and corresponding cell coordinates.
- Analyze the plateau phase (Figure 7C). Detect individual oscillations by thresholding the raw data or by thresholding the first derivative of the time-series data. Define the beginning and end of an individual oscillation as the time corresponding to the oscillation's half amplitude.
- Calculate the duration and the frequency of individual oscillations for each cell. Calculate the inverse value of the interspike interval (suitable for regular activity patterns). Alternatively, divide the number of oscillations by the time interval of the record (suitable for irregular activity patterns).
- Calculate the active time. Express the active time as the sum of durations, and divide this value by the time interval. Alternatively, multiply the frequency and the duration that correspond with an oscillation.
NOTE: Dividing the sum of durations by the time interval provides robust results, but has low statistical discrimination as a single data point per cell is obtained. Multiplying the frequency and duration of an oscillation provides an oscillation-to-oscillation temporal resolution.
The injection of the agarose solution into the pancreatic duct is the most critical step in pancreas tissue slice preparation. A successful injection can be recognized by a whitening of the pancreas tissue, as seen on the left side of Figure 3A, while an incompletely injected part of the pancreas is presented on the right side of Figure 3A. The islets of Langerhans can be recognized by the naked eye or under a stereomicroscope, and this aids in cutting the appropriate parts of the pancreas for subsequent embedding in agarose blocks (Figure 3B). In a freshly cut mouse pancreatic tissue slice, islets of Langerhans can be easily distinguished from the surrounding exocrine tissue and mesenchyme as white spots under the stereomicroscope (Figure 3C) or as brownish structures under the light microscope (Figure 3D). The pancreatic tissue slices can be used for distinct types of experiments for at least 12 h after slicing. In addition to the gross morphological assessment under the stereomicroscope, the light microscope, and the functional responses of cells during calcium imaging, the viability of the pancreatic tissue slices can be assessed (Figure 4).
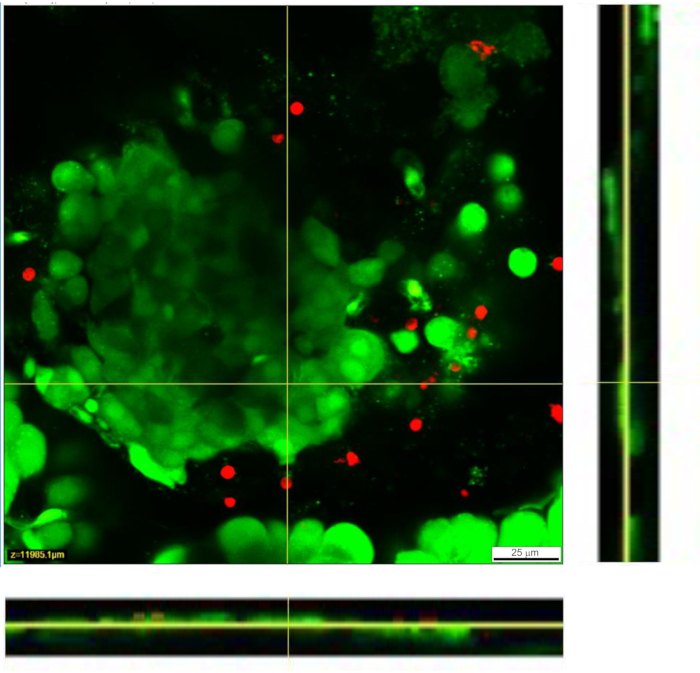
Figure 4: Viability of cells within the tissue slice. Viability of cells was determined with the Live/Dead assay. Live cells are stained by Calcein AM (shown in green), while dead cells are stained with ethidium homodimer-1 (shown in red). Yellow lines denote the position of the X-Y cross section of the Z-stack displayed at the bottom and the right. The full depth of the Z-stack is 88 µm. Please click here to view a larger version of this figure.
For calcium imaging experiments, the fluorescent calcium indicator needs to penetrate through a few layers of cells. Figure 5A presents successful loading of the cell-permeable Ca2+ indicator dye into the pancreatic tissue slice in which individual islet and acinar cells can be recognized. In contrast, slices in Figure 5B–D are not optimal due to unsuccessful penetration of the dye (Figure 5B), lack of islet cells (Figure 5C), and a lot of necrotic tissue on the surface (Figure 5D). Such slices can be discarded, checked for the presence of additional islets that are cut or stained better (see Table 1 for troubleshooting), or used for recording the responses of exocrine cells.
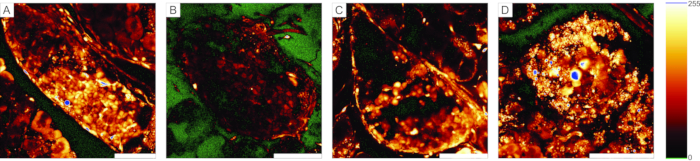
Figure 5: Examples of usable and unusable preparations. (A) An example of a successful preparation of the pancreas tissue slice with well-stained cells in the islets of Langerhans, as well as ductal cells and surrounding acinar tissue. (B) An example of a poorly stained tissue slice. (C) Example of an islet of Langerhans with structural discontinuations. (D) An example of an islet of Langerhans containing many dead cells and a lot of debris. The "glow-over, glow-under" lookup table on the right displays 0 intensity in green and saturation in blue. Scale bar = 100 µm. Please click here to view a larger version of this figure.
Representative results from calcium imaging using the cell-permeable Ca2+ indicator dye are shown in Figure 6. In Figure 6A, a high-resolution image of a pancreatic tissue slice is presented, containing an islet of Langerhans, acinar tissue, and a pancreatic duct. For better distinction, the endocrine, exocrine, and ductal part of the pancreatic tissue slice presented in Figure 6A are colored in Figure 6B. Using appropriate stimuli can functionally discriminate between different islet cells, or islet and non-islet cells51. Beta cells will typically respond to a square-pulse stimulation by glucose with a transient increase in [Ca2+]IC followed by fast calcium oscillations on a sustained plateau (Figure 6C, upper panel).
As all beta cells are coupled into a single, large, functional syncytium, these oscillations are also very well synchronized among different cells by means of spreading [Ca2+]IC waves32,34,52,53,54 (Figure 7C). Slower [Ca2+]IC oscillations with a period of 5-15 minutes may underlie the fast oscillations or even be the predominant type of reponse55,56. The same simple protocol may reveal other types of responses, especially at the periphery of islets (Figure 6C, lower panel). As these cells are not synchronized with beta cells and respond with faster and more irregular oscillations that are already present in low glucose conditions or with a decrease in activity, such responses are highly suggestive of non-beta cells21,32,57,58. However, their definitive functional characterization requires more complex protocols with additional stimulation steps or alternative approaches, which are discussed below. Typical responses of acinar and ductal cells are presented in Figure 6D and Figure 6E, respectively. Refer to the literature for more details on acinar and ductal cells22,23,35.
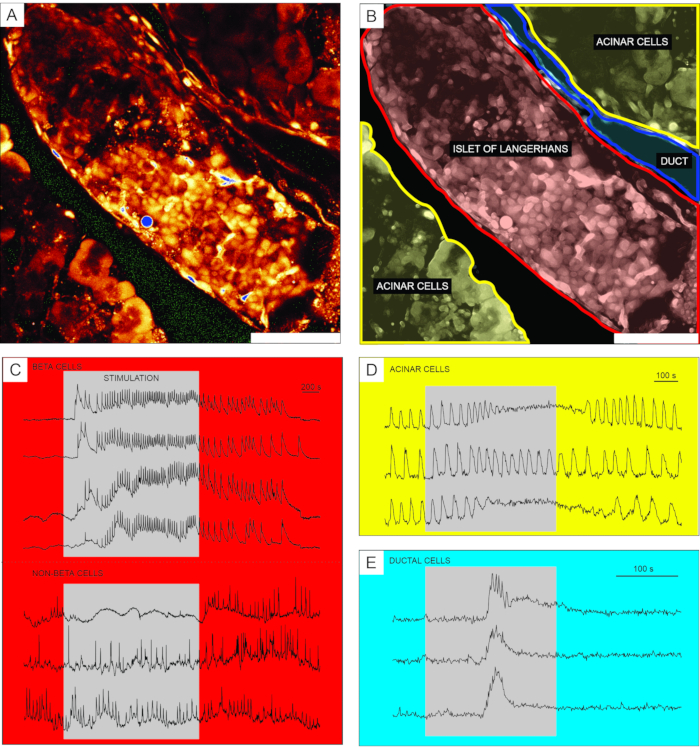
Figure 6: Representative results of calcium dynamics in distinct types of pancreatic cells. (A) A high-resolution image of an islet of Langerhans with surrounding tissue. Scale bar = 100 µm. (B) Delineation of distinct parts of pancreatic tissue with acinar tissue shown in yellow, an islet of Langerhans shown in red, and a segment of the ductal tree in blue. Scale bar = 100 µm. (C) Typical traces of calcium dynamics in beta and putative non-beta cells during stimulation with 12 mM glucose; 3 mM glucose was used for non-stimulatory conditions. Protocols that can be used for more specific discrimination of non-beta cells are described in the discussion section. (D) A typical trace of calcium dynamics of acinar cells stimulated by 25 nM acetylcholine. (E) A typical trace of calcium dynamics of ductal cells stimulated by 1 mM chenodeoxycholic acid. Please click here to view a larger version of this figure.
After successful calcium imaging, the data are first exported and corrected for bleaching by a combination of an exponential and linear fit, as described in the protocol section. A time series before and after bleaching correction is presented in Figure 7A. Thereafter, several parameters in the activation and deactivation phase of the response as well as the plateau phase can be analyzed. A delay in the onset of [Ca2+]IC increase after stimulation can be measured as represented by delayA di Figure 7B and the heterogeneity in delays among individual cells (delayA1). The same parameters (delayD and delayD1) can be used to describe the deactivation phase. Following the initial transient [Ca2+]IC increase, the plateau phase in most pancreatic beta cells in an islet is characterized by relatively regular high frequency [Ca2+]IC oscillations. The plateau phase can be described by analyzing the classical functional parameters. The schematic presentation of [Ca2+]IC oscillations duration, frequency, and percentage of active time are presented in Figure 7C. In calcium imaging with acquisition rates higher than 10 Hz, calcium waves repeatedly spreading across the islet can also be recognized clearly (Figure 7C).
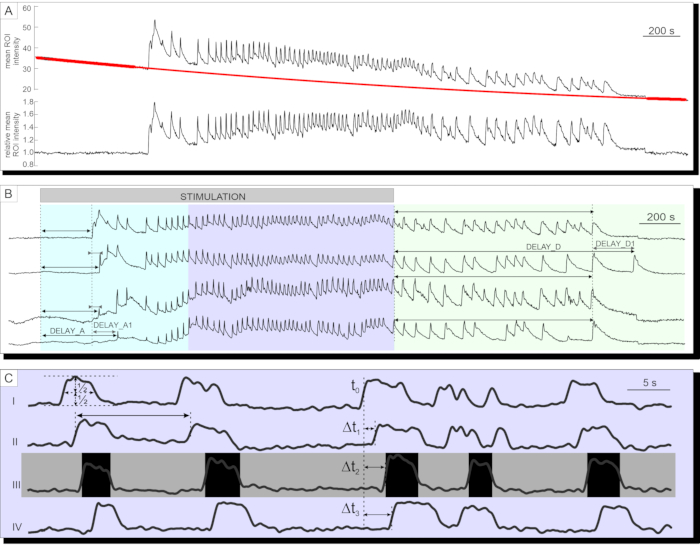
Figure 7: Analysis of time-series data. (A) Correction of time-series data for photobleaching. (B) Analysis of delays to activation after stimulation and to deactivation after cessation of stimulation with 12 mM glucose. Duration of stimulation is denoted by the light gray, shaded bar in the image. (C) Analysis of several parameters of the plateau phase: I) Duration of the oscillation determined at half-height, II) frequency of oscillations determined by inter-oscillation intervals. III) active time as a product of frequency and duration of oscillations. I-IV) Delays between oscillations in any given wave of oscillations that spread across the islet of Langerhans determined by the delays (Δt) in time at which a single cell reaches half-height of the oscillation. Please click here to view a larger version of this figure.
