Anastomosis of the pulmonary artery to the pressurization tubing is shown in Figure 1A. Following the application of hydrostatic pressure, the pulmonary trunk distends radially (Figure 1B) indicating that the pulmonary valve leaflets are in a closed configuration. Pulmonary valve conformation was confirmed by µCT. In this case, the leaflets were coapt (closed) and the annulus was circular (Figure 2A). Figure 2B,C shows varying degrees of inadequate pulmonary valve pressurization by either fixation (Figure 2B) or arterial collapse (Figure 2C).
Sample block trimming was guided by the µCT volume rendering. In this case, the plane parallel to the sino-tubular junction was chosen as the slicing direction. Using anatomical landmarks, the µCT volume rendering virtual cross sections was correlated with optical images (Figure 3) to confirm the slicing direction and location.
Once the specimen block was at the desired location and orientation, high-resolution SBF-SEM images were taken at a local region within a leaflet. Image correlation was done between the µCT volume rendering virtual slice (Figure 4A), low-resolution SBF-SEM images (Figure 4B), and high-resolution SBF-SEM images (Figure 4C). Because of the manual sample mounting, requisite slices of the specimen block were needed to create a flat surface before acquiring images in the SBF-SEM; hence, the different locations between Figure 3 and Figure 4.
A full image correlation between µCT and SBF-SEM data sets can be seen in Video 1. The pulmonary valve specimen in the µCT volume rendering can be easily discerned from the surrounding embedding resin because of the staining of heavy metal atoms. Lengths and angles are measured in the image to guide the slicing. In this example, the plane parallel to the sino-tubular junction was used. A virtual slice through emulates the removal of the material until the depth of interest is reached. High-resolution images taken by SBF-SEM were taken at this cross section and registered to the µCT data set.
Once acquired, high-resolution images taken by SBF-SEM can be imported into an image processor and compiled into a 3D representation (Figure 5) where extracellular components can be identified.
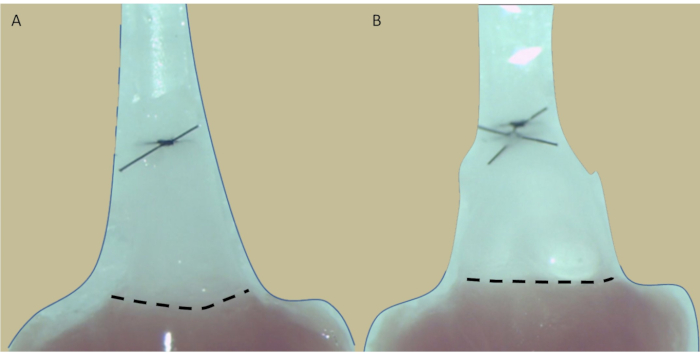
Figure 1: Representative images of anastomosed pulmonary trunk. The excised pulmonary trunk (A) before and (B) after hydrostatic pressurization. The dotted line indicates the ventriculo-arterial junction where the annulus of the pulmonary trunk resides. Note the pulmonary trunk distention upon pressurization. Please click here to view a larger version of this figure.
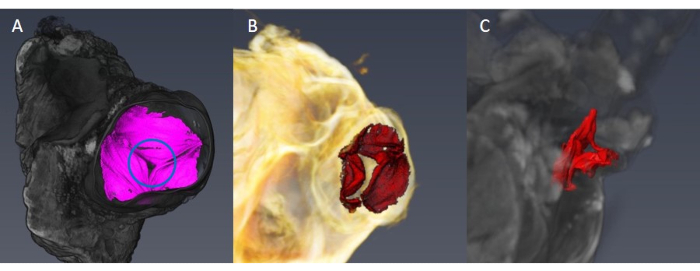
Figure 2: Representative µCT volume rendering pulmonary valve. (A) The pulmonary valve is in a closed position with the leaflets adequately stretched and coapt (circle). (B,C) Inadequate pressurization of the pulmonary valve. Note that the leaflets are not properly coapt (B) and that the annulus is not circular (C). Please click here to view a larger version of this figure.
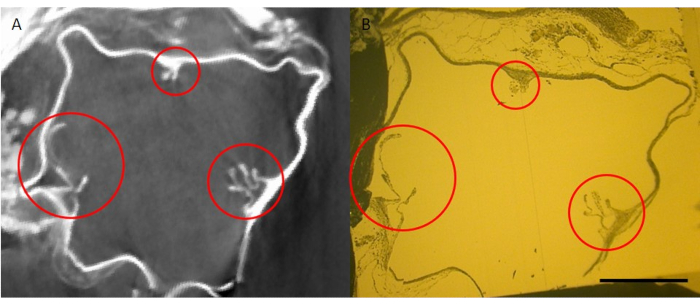
Figure 3: Image correlation of pulmonary valve specimen block. (A) µCT volume rendering virtual slice and (B) physical specimen block after trimming taken by optical microscopy. Sections of pulmonary valve leaflets are circled in red and were used as landmarks to correlate the two different imaging methods. Scale bar corresponds to 500 µm. Please click here to view a larger version of this figure.
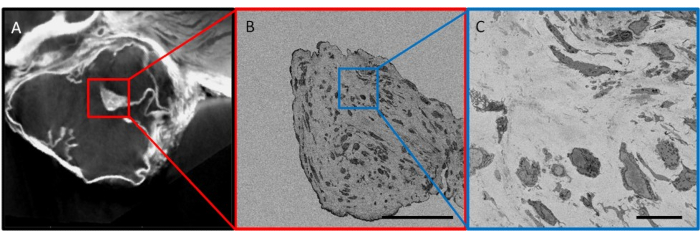
Figure 4: Image correlation of imaged pulmonary valve cross section. (A) Virtual cross section generated by µCT volume rendering. Red box indicates the region that was imaged using SBF-SEM in (B). (B) Low-resolution overview images to correlate with µCT cross section. Blue box represents the location of (C) high-resolution SBF-SEM imaging. Scale bars correspond to (B) 100 µm and (C) 10 µm. Please click here to view a larger version of this figure.
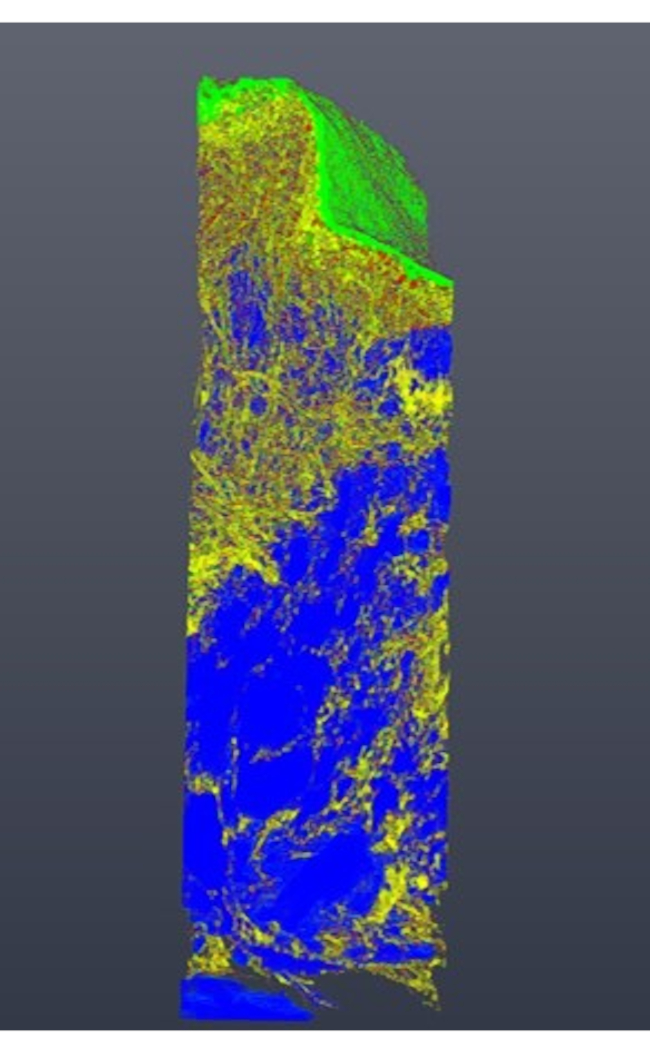
Figure 5: Segmented region of the pulmonary valve taken by SBF-SEM. Cross-sectional images were stacked and compiled to form a 3D representation of a local pulmonary valve region. Labels were assigned to endothelial cells (green), valvular interstitial cells (blue), and extracellular fibers (yellow). The approximate dimensions of the imaged region are 30 µm x 20 µm x 100 µm. Please click here to view a larger version of this figure.
| Tube potential | 70 kV |
| Tube current | 75 μA |
| Focus mode | M |
| Trajectory | Circular |
| Projections/Revolution | 2880 |
| Mode | 3040 x 3040 px |
| Averaging | 1 |
| Exposure time | 1.0 s |
| Sample-to-gun distance | 15 mm |
| Detector-to-gun distance | 725 mm |
| Voxel size | 2.9 μm |
| Field of view | 8.4 x 8.4 x 6.3 mm |
Table S1: Imaging parameters for µCT.
| Landing energy | 2 – 2.5 kV |
| Beam current | 100 – 400 pA |
| Working distance | 6.5 – 7 mm |
| Detector | VS-DBS |
| Dwell time | 1 – 2 μs |
Table S2: Imaging parameters for SBF-SEM.
Video 1: Image correction of µCT and SBF-SEM data sets. Please click here to download this Video.
