All animals received humane care in accordance with the NIH Guide for the Care and Use of Laboratory Animals. The Institutional Animal Care and Use Committee (IACUC-protocol 2017N000184) and Animal Care and Use Review Office (ACURO) approved all animal protocols. Inbred male Lewis rats (250-400 g) were used for all experiments.
1. Surgery
- Anesthetize the Lewis rats using isoflurane inhalation. Induce anesthesia with 5% isoflurane in the induction chamber, and maintain anesthesia with 1.5-3% isoflurane inhalation through a breathing cone.
- Apply eye lubricant before surgery in survival procedures. Shave the surgical site, treat with depilatory cream, scrub, and drape with sterile drapes.
- Confirm total anesthesia with a toe pinch test before incision and regularly during the procedure. Monitor heart and respiratory rates throughout the entire procedure. For all surgeries, maintain sterile conditions by using sterile instruments, supplies, drapes, and gloves. See the Table of Materials for the list of instruments used for the procedures.
2. Donor right partial hindlimb procurement
- Make a circumferential incision of the skin above the ankle at the distal third of the leg.
- Skeletonize and cauterize the saphenous artery and the terminal branch of the popliteal artery using bipolar forceps. Cauterize and cut off the gastrocnemius, soleus, tibialis anterior, and biceps femoris muscles until the tibial bone is exposed.
- Make a 2.5 cm incision at the right inguinal crease. Dissect out the inguinal fat pad and retract it distally to expose the femoral vessels. Use a fishhook retractor to grasp the inguinal ligament and clamping forceps to hold the inguinal fat pad distally.
NOTE: The inguinal fat pad is included in the harvest of the partial limb. - Dissect the femoral vessels, individualize Murphy branches (deep muscular collateral branches usually located halfway between the inguinal ligament and the epigastric branch), and ligate with 8-0 nylon ties.
- Heparinize the donor rat with 100 IU/kg heparin, injected in the penile dorsal vein using a 27.5 G needle.
- Complete the skin incision around the hip.
- Cauterize the biceps femoris and gluteus superficialis muscles using bipolar forceps. Cauterize and cut the sciatic nerve at mid femur length. Expose the femur proximally at the level of the posterior femoral crest.
NOTE: Adductor and quadriceps muscles are left out of the procurement. The innominate pedicle is preserved. - Ligate femoral vessels with 8/0 nylon ties at the level of the inguinal ligament. Perform an arteriotomy on the femoral artery just below the ligature and dilate to allow for the insertion of a 24 G angio-catheter.
- Cauterize and cut remaining muscle underneath the pedicle, exposing the anterior side of the femur.
- Cut the tibia and femur using a bone cutter as proximally and distally as possible, respectively (mid-length).
- Flush the partial hindlimb with 2 mL of heparin saline (100 IU/mL) to obtain a clear venous outflow. Store on ice in a sterile gauze until microvascular transfer (Figure 1).
- While the animal is under general anesthesia, perform euthanasia by exsanguination. Confirm death by absence of respiratory movement and heartbeat.
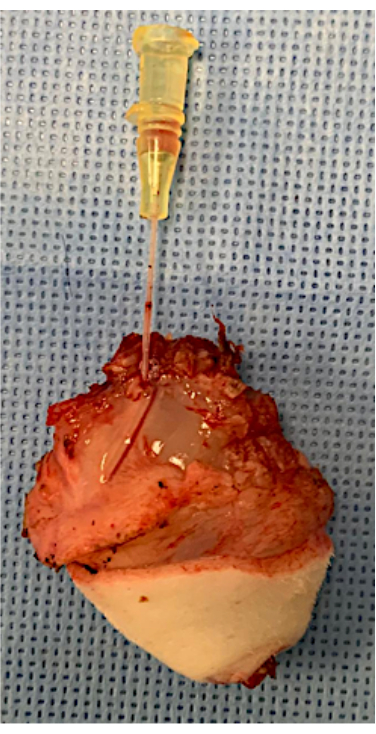
Figure 1: Rat partial hindlimb harvested. A 24 G angiocath is inserted in the femoral artery, ready for heterotopic microvascular transfer. Please click here to view a larger version of this figure.
3. Recipient surgery
- Before the incision, shave the back of the neck, and administer buprenorphine 0.01-0.05 mg/kg subcutaneously. Place the rat in a supine position on a heating pad.
- Make a 2.5 cm incision in the right inguinal crease. Dissect the inguinal fat pad and recline it distally to expose the femoral vessels. Use a hook to retract the inguinal ligament and clamping forceps to hold the inguinal fat pad distally.
- Dissect the femoral vessels, individualize the Murphy branches, and ligate with 8/0 nylon ties.
- Ligate both vessels above the epigastric vessels using 8/0 nylon ties. Place approximator clamps proximally and dilate vessel ends; rinse with heparin saline.
- Make an incision on the left flank above the hip, and create a subcutaneous pocket with a subcutaneous tunnel to the inguinal crease.
NOTE: The inset incision is made above the range of motion of the hip to ensure that the animal maintains a normal hindlimb motion. Additionally, keeping a cutaneous bridge between the graft inset and the microvascular transfer site allows for better fixation of the graft (Figure 2). - Place the proximal part of the partial limb and the inguinal fat pad through the subcutaneous tunnel for microvascular transfer. Perform venous and arterial anastomoses using 10/0 nylon sutures. Remove both approximator clamps, and observe revascularization of the limb. Perform a "milking test" on both vessels to assess the patency of each anastomosis.
NOTE: Eight to nine sutures are usually necessary for venous anastomosis, 6 sutures on average for arterial anastomosis. - Make a longitudinal skin incision on the medial side of the transplanted limb, and insert the graft. Remove excess skin of the graft, and close the wound with separate sutures and a running suture using absorbable 4/0 sutures.
- Suture together the inguinal fat pads of the transplanted limb and the recipient using two separate absorbable sutures, and close the inguinal crease at the very end after a last checkup of the microvascular anastomoses.
NOTE: Inguinal fat pads are sutured tightly to add a protective layer of fat above the anastomoses and ensure a secured position of the graft and its pedicle. A meticulous closure is better for wound healing; it also prevents residual bleeding from the wound and decreases the risk of self-mutilation. - Compensate fluid loss subcutaneously with 1-3 mL of saline according to the amount of perioperative bleeding.
- Place an Elizabethan collar around the neck of the animal, and apply 2 loose sutures to the skin to maintain it in the correct position.
- Stop isoflurane inhalation, and monitor the animal continuously on a warming pad until fully conscious and ambulatory.
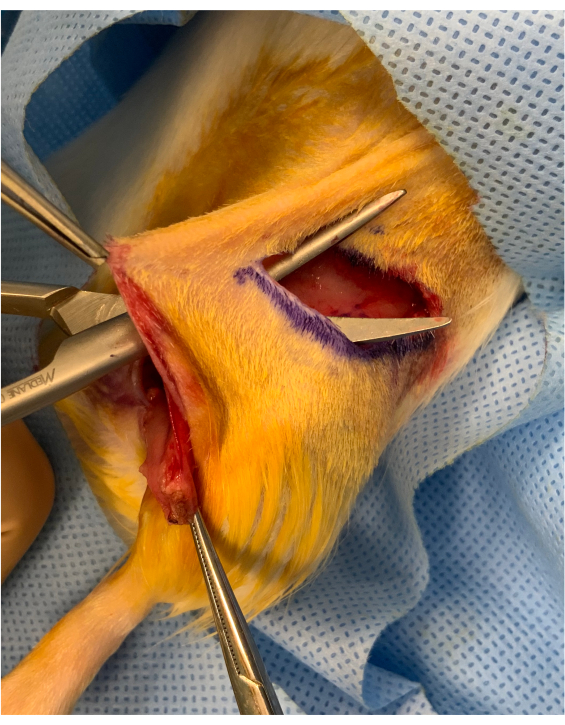
Figure 2: Perioperative image before inset of the osteomyocutaneous limb. A cutaneous bridge of approximately 1 cm is preserved between the inguinal crease incision and the inset of the graft above the hip. The graft is placed under the bridge, maintaining it steady for microvascular transfer. Please click here to view a larger version of this figure.
4. Postoperative care
- Monitor the animal twice daily for 72 hours, then once daily until postoperative day (POD) 7, and then twice per week.
NOTE: Monitoring must be adjusted to the animal and graft condition (pale eyes might require supplementary fluids, porphyrin staining as an indicator of animal pain, abnormal graft color/temperature), and further care should be discussed with the veterinarian. Single housing is required for the recipient rats during the entire study period to avoid any damage to the graft. - Perform analgesia with subcutaneous injection of buprenorphine and/or non-steroid anti-inflammatory drug according to IACUC guidelines.
- Evaluate the graft, and perform physical examination daily with pictures using the same device.
NOTE: Using hair removal cream on the graft's skin is helpful to better assess the skin color of the transplant.
In this single-operator study, 30 syngeneic heterotopic partial limb transplants were performed. Success was defined at postoperative day 21 as the absence of VCA failure or complications requiring euthanasia. The normal evolution of the graft is represented in Figure 3. The mean duration for partial limb procurement and graft inset in the recipient were 35 and 105 min, respectively; the mean ischemia time was 105 min. During follow-up, two types of complications occurred (Table 1)-early or late. Some required euthanasia, others were salvaged, all were discussed with staff veterinarians (Table 2). This study reports the authors' experience and advice for beginners in rodent microsurgery (Supplementary Table 1).
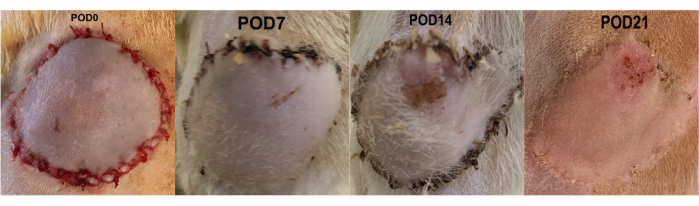
Figure 3: Normal evolution of the heterotopic hindlimb model until the end of the study. Hair regrowth is observed during the first postoperative week; cutaneous retraction appears after 2 weeks. Abbreviation: POD = postoperative day. Please click here to view a larger version of this figure.
Management of perioperative complications
Arterial or venous thrombosis is the most common perioperative complication. The most important tip to overcome this and turn the surgery into a success is to make an early diagnosis, i.e., continuous monitoring of the flap color/bleeding and recurrent patency test are fundamental before closing the anastomoses surgical site. The prevention of this complication should be in the surgeon's mind as soon as an incision is made. The donor should be heparinized with IV injection of heparin 100 IU/kg 5 min prior to graft arterial ischemia. Once harvested, the graft should be flushed with heparin saline (100 IU/mL) until venous outflow is clear. In this study, perioperative arterial thrombosis happened in 10% of cases.
Bleeding is a less frequent occurrence and is easily mitigated with a cautious cauterization of the graft muscles and a thorough dissection of the recipient site. The primary cause of bleeding is the anastomotic leak in the artery. This should resolve by itself within 3 min, or if not, re-clamping and revision of the leaking anastomosis are necessary. Anesthesia-related complications, which occurred in 6.7% of cases, are more frequent with untrained microsurgeons. Using isoflurane is a reliable way to anesthetize rats, and the length of anesthesia can be adjusted in real time. The surgeon must be trained to use the machine correctly, follow the guidelines for induction and maintenance regimen, and closely monitor the heart and respiratory rates throughout the operation. Depending on the species, age, or weight of the animal, the amount of isoflurane needed may vary. Unpredictable animal loss is a rare event and is usually not explained by an anesthetic or surgical mistakes.
Early complications (<POD7)
VCA failure can occur during the first postoperative week due to microvascular thrombosis (venous thrombosis more frequent than arterial). Perioperative pedicle inset at the groin level is a very important step. Moving the rat's hindlimb to mimic the movement's effect on the pedicle is crucial; the pedicle should never be too loose nor too tight. Intensive monitoring is a fundamental requirement, as necropsy must be performed as soon as a VCA failure diagnosis is made. During necropsy, an analysis of the position of the pedicle (kinking or tension) and quality of the thrombosed anastomosis (back wall suture, intraluminal flap) provides much information on what can be improved during the next procedure and thus, should be performed by the operating surgeon. Venous thrombosis was a cause of early euthanasia in 20% of cases, all of which occurred before POD5 (Figure 4).
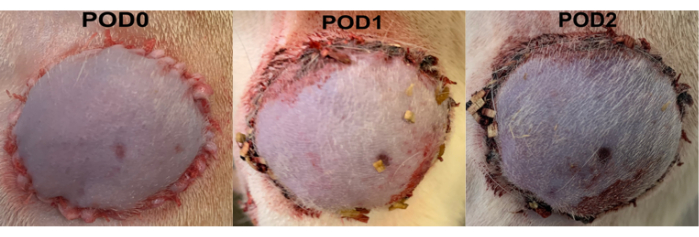
Figure 4: Postoperative venous thrombosis. The skin appears blue and becomes darker each day. Abbreviation: POD = postoperative day. Please click here to view a larger version of this figure.
Self-mutilation (or autophagia) is a serious concern in non-sensate grafts; it often occurs between POD2 and POD7. If limited to less than a third of the graft surface and concerning only skin, surgical debridement and suture using non-absorbable sutures can be discussed with the staff veterinarian (Figure 5A–C). In such case, non-absorbable sutures should be removed under sedation after 10-14 days. Prevention relies on the use of an E-collar stitched to the neck15 until POD7 and the cleaning of any blood or crust on the animal's surgical wounds. Repeated autophagia or deep mutilation requires euthanasia (Figure 5D).
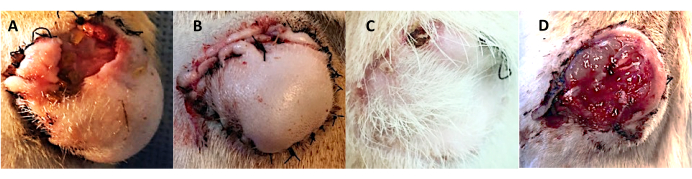
Figure 5: Postoperative self-mutilation of the non-sensate graft. (A–C) The limited surface of auto-mutilation at (A) POD2. (B) Surgically debrided and re-sutured; (C) aspect at POD21. (D) Severe autophagia of multiple layers of the graft leading to euthanasia of the animal. Abbreviation: POD = postoperative day. Please click here to view a larger version of this figure.
Late complications (>POD7)
Less frequent and less lethal, these complications demand veterinarian consultation to provide adequate treatment. First, bone exposure can be observed in this model, usually after initial healing on the third week post-operation. Prevention is based on careful bone-cutting (use of bone cutter creating smooth edges); covering the bone edges with surrounding muscles while accounting for later muscle atrophy is helpful. If detected early and the animal is in good condition, surgical revision can be discussed with the veterinarian. Second, dermal cysts can occur around the surgical site after two weeks (Figure 6). They usually do not interfere with the rat's or the graft's condition, but can fistulize to the skin and get infected. Washing the surgical site of the graft inset to avoid any residual hair in the wound prevents the creation of the cyst. The indication for surgical drainage can be evaluated with the veterinarian.
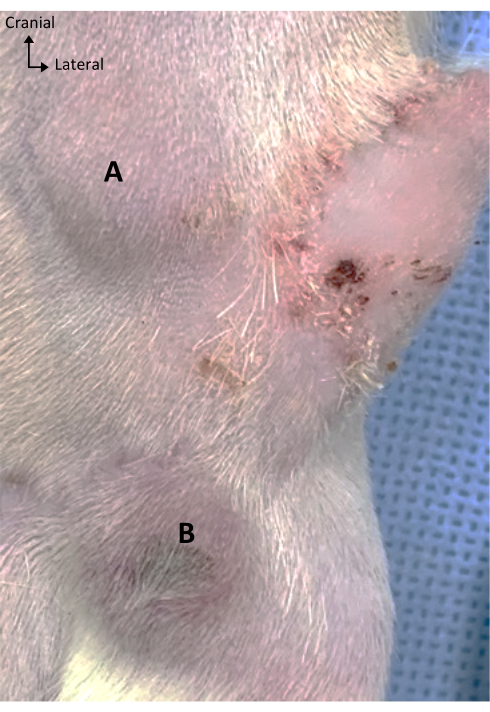
Figure 6: Dermal cysts. Dermal cysts appearing(A) after POD14, (B) sometimes with a cutaneous necrotic center prior to the fistula. Abbreviation: POD = postoperative day. Please click here to view a larger version of this figure.
| Complication | Solution | Prevention | |
| Peri-operative | Microvascular thrombosis | Re-do the anastomosis rapidly after rinsing the vessel ends with heparin saline and attesting good flow. | Heparinize the donor, flush the flap, master the anastomosis technique, and use adequate instruments and suture. |
| Bleeding | Cauterize if from muscles, reclamp if from the anastomosis and not stopping spontaneously within 3 min. | Thorough cauterization during graft harvest | |
| Anesthesia-related death | Discuss the encountered problem with vet staff. | Training in use of anesthesia machine and perioperative rat monitoring | |
| Early (<POD7) | Microvascular thrombosis | Early euthanasia and necropsy to reveal the cause of thrombosis | Depends on the cause |
| Auto-mutilation | Discuss surgical repair with the vet if first event and superficial damage to the graft. | E-collar from POD-2 to POD7 | |
| Late (>POD7) | Bone exposure | Discuss surgical revision with the vet. | Cut the bone with bone cutter, make sure the edge is smooth, recover with surrounding muscles, account for later muscle atrophy (cut short). |
| Dermal cyst | Discuss surgical drainage and antibiotic treatment with the vet | Wash the inset site with water; avoid leaving any hair in surgical site. |
Table 1: Potential outcomes. Prevention and solutions.
End of study
The end of the study in this model was set at POD21; animals were euthanized using CO2 asphyxiation or by exsanguination. As a non-functional graft, muscle atrophy and fatty degeneration were observed as consequences of the lack of reinnervation. Biopsies of the skin and muscle are saved for histological analysis. The inguinal crease is reopened for the evaluation of the vascular pedicle (placement, patency) if euthanasia is performed before the end of the study.
| Five reasons for consulting the staff veterinarian |
| 1) Before the start of the study to inform her/him of the nature of your study, planned analgesia, and follow-up strategies and expected outcomes |
| 2) Special diet or supplementary nutrients that can help improve the animal condition during the study |
| 3) Unexpected anesthesia-related death |
| 4) Unexplained worsening of the animal condition |
| 5) Surgical complication to assess salvaging possibilities or indications for euthanasia |
Table 2: When to call the vet. Communication with the staff is essential for the conduct of an in vivo study.
Supplementary Table 1: "Dos & Don'ts." Advice for young microsurgical trainees. Please click here to download this Table.
