All procedures were approved by the Institutional Review Board at the Medical University of South Carolina and conformed to the Declaration of Helsinki.
1. Participant recruitment
- Recruit individuals post-stroke from the local database. For this experiment, 16 individuals were recruited from a local electronic recruitment database. In some instances, participants were recruited specifically because they had failed to respond to TMS at rest in previous studies performed by our research group.
- Use the following inclusion criteria for this investigation: males and females between the ages of 18-85, at least 6 months post-stroke, residual paresis of the lower extremities, and able to stand 10 min without an assistive device.
- Exclude participants if they had a history of seizures, took prescription medications that lowered seizure thresholds, had a history of brain injury and/or other diseases of the central nervous system, had implanted devices or metal objects in their head, or had severe arthritis or orthopedic conditions limiting their passive range of motion.
NOTE: Participants' demographics are located in Table 1.
| Study ID | Age | Months post Stroke |
Sex | Race | Type of Stroke | Stroke Hemisphere |
Altezza (cm) |
Weight (kg) |
Self-Selected Walking Speed (m/s) | Walking Aid |
||
| 1 | 67 | 28.7 | M | C | Intracerebral Hemorrhage | Right | 180 | 74.8 | 0.61 | None | ||
| 2 | 84 | 55.8 | F | C | Ischemic | Right | 165 | 68.0 | 0.94 | None | ||
| 3 | 56 | 262.7 | F | C | Subarachnoid Hemorrhage | Left | 152 | 59.0 | 1.29 | None | ||
| 4 | 67 | 141.8 | M | C | Intracerebral Hemorrhage | Right | 180 | 72.6 | 0.27 | Cane / AFO | ||
| 6 | 48 | 21.6 | M | C | Intracerebral Hemorrhage | Right | 170 | 61.2 | 0.83 | None | ||
| 7 | 58 | 93.9 | M | C | Acute Ischemic | Left | 168 | 112.5 | 0.77 | Quad Cane / AFO | ||
| 8 | 71 | 55.3 | F | AA | Acute Ischemic | Left | 170 | 68.0 | 1.05 | None | ||
| 9* | 65 | 23.7 | M | C | Acute Ischemic | Right | 178 | 84.8 | – | Knee Brace | ||
| 10 | 70 | 26.6 | M | C | Acute Ischemic | Left | 173 | 78.9 | 0.81 | None | ||
| 12 | 70 | 10.0 | M | C | Acute Ischemic | Left | 170 | 86.2 | 1.11 | None | ||
| 13 | 65 | 80.6 | M | C | Acute Ischemic | Right | 185 | 139.7 | 0.93 | Cane / Crutch | ||
| 14 | 79 | 83.0 | M | C | Acute Ischemic | Right | 175 | 88.5 | 0.48 | Cane | ||
| 15 | 51 | 54.4 | M | AA | Acute Ischemic | Left | 178 | 90.7 | 1.35 | None | ||
| 17 | 65 | 18.5 | M | C | Acute Ischemic | Right | 170 | 74.8 | 0.28 | Cane | ||
| 18 | 63 | 48.8 | F | AA | Acute Ischemic | Right | 170 | 83.9 | 1.12 | None | ||
| 19 | 58 | 25.9 | M | C | Acute Ischemic | Both | 183 | 88.5 | 1.10 | None | ||
| * Participant removed from data analysis due to inability to complete required assessments | ||||||||||||
| AFO = ankle foot orthortic | ||||||||||||
Table 1: Participant demographics.
- Make initial contact with participants via phone and briefly explain the testing procedures. Invite interested individuals to the laboratory.
- Upon arrival to the research facility, have a member of the research staff fully explain the experimental protocol to the prospective participants.
- When a prospective participant confirms their willingness to participate in the study, obtain written informed consent approved by the local institutional review board.
2. Image guidance system and participant setup
- Utilize image guidance software to ensure consistent delivery of the TMS pulses during the assessment.
- Start a new project using the MNI head model native to the image guidance system. Open the software and select New MNI Head Project.
- In the pop-up window, click on the Targets tab and then click Configure Targets. Determine the scalp location directly superior to the pre-central gyrus and 0.5 cm lateral to the midsagittal line.
- Once the location is visually identified, add a new rectangular grid by clicking on the Nuovo, and then on the Rectangular Grid. The grid should appear on the screen, and the medial row should be 0.5 cm lateral to the midsagittal line.
- Resize the grid by typing 3 and 5 in the grid size boxes. Set the grid spacing to 10 by 10 mm by typing in the grid spacing boxes. Select the Cursor Tool, and then move the cursor to the scalp image.
- Press and hold the mouse button to rotate the scalp image to ensure all grid points are touching the skin. If the grid points are not on the scalp, adjust the curvature of the grid by moving the curvature slider.
- Repeat these procedures to place another 3 x 5 grid over the opposite hemisphere.
NOTE: This can be performed before a participant's enrollment into the study and arrival to the laboratory. Additionally, a participant's anatomical T1-weighted image can be used if available. Specific details on using anatomical MRIs for navigation can be found in the previously published article16.
- Start a new session within the image guidance software by selecting the Sessions tab once the software is open.
- Click on Nuovo, and then on Online Session. In the next window, select the two grids created in the previous section (section 2.1) by clicking on them, and then click on Add.
- In the IOBox tab, under TTL Trigger Options check the box next to Use Switch (Switch In) and input 0 ms into the Dead Time box. Click on the Next button at the top. Visually ensure the image guidance system's camera is active.
- Begin participant registration by placing the subject tracker, supplied with the image guidance system, around the participant's forehead.
- Manually adjust the camera to ensure the participant tracker is in the middle of the camera's field of view. Next, click on the Registration tab at the top of the software.
- Place the image guidance system's pointer/marker onto the registration landmarks: nasion and the right and left periauricular points. When the pointer is placed on the skin, click on the Next button to register the participant's skin locations to the image guidance software.
- After the registration landmarks have been captured, click on the Scaling tab at the top of the software window. Place the pointer on the rightmost, leftmost, topmost, frontmost, and backmost locations of the participant's scalp.
- Click on the Next button at each location to scale the image guidance system to the participant's head. After scaling is complete, click on the Perform tab at the top of the software. The image guidance system is now ready.
3. Surface electromyography preparation and setup
- Prepare the participants' tibialis anterior (TA) and soleus (SOL) muscles for surface electromyography (sEMG) electrodes. To prepare the skin for sEMG, clean the area using alcohol pads and, if necessary, remove any hair with a single-use safety razor. Place the sEMG disposable gel electrodes according to SENIAM guidelines17.
NOTE: Sensor placement for the TA is 1/3 of the way down on the line between the tip of the fibula and the tip of the medial malleolus. For the SOL, place the sensor 2/3 of the line between the medial condyle of the femur to the medial malleolus. - Once the electrodes are attached, visually inspect the signal for quality. Then, proceed to wrap the shanks with an elastic bandage to minimize any movement of the electrodes and the resultant artifact during testing.
NOTE: Record sEMG signals at 5000 Hz in a 0.5 s window starting 0.1 s before the delivery of the TMS pulses. The exact sampling frequency and amount of data collected will be dependent on the hardware and software used to record the sEMG response to TMS. For details on establishing EMG recordings and analyses see Tankisi et al.18.
4. Force plate and participant safety setup
- Open the data collection software and start a new trial to calibrate the dual-top force plate.
- Click Start and begin an FP Zero trial. Collect 3-5 s of data with no load on the force plate, and then click Stop.
- Once the force plate is calibrated, the participant has been registered to the image guidance system (section 2.2), and the sEMG electrodes have been placed and tested for the signal quality (section 3), instruct the participant to stand and fit them with a safety harness.
- Have the participant step onto the force plate and standardize their foot placement with masking tape pre-applied to the force plate to signify the foremost position of the foot and medial edges of the feet equal distances from the midline.
- Attach the participant's safety harness to the ceiling support. Place a rollator, or similar device, around the force plate to provide participants with something to steady themselves with during testing if needed.
NOTE: Ensure that during all standing TMS procedures the participants are secured to the ceiling via a safety harness to prevent a fall.
- Measure and collect the participant's weight as they stand on the force plate by clicking Start and selecting an FP Static trial. Record 2-5 s worth of data and click Stop to end the trial.
- When standing on the force plates, ensure that the data collection software displays two bar graphs representing the weight/force under each of the participant's feet (Figure 1A). When the participant shifts their weight to one side, the bar graphs will change in height (Figure 1B).
- If a participant unloads the weight on their legs to their arms, ensure the bar graph display changes color (Figure 1C). After a participant becomes comfortable standing with equal weight distributed between their legs, measuring the CMR can commence.
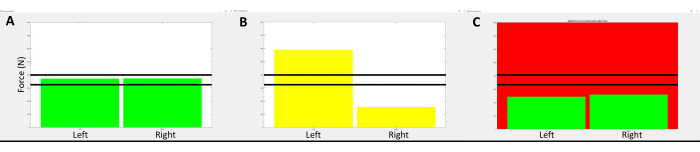
Figure 1: Representative image of the visual feedback provided to participants during the standing TMS assessment. (A) displays the visual feedback given to participants while they were standing with their weight equally distributed between the paretic and non-paretic legs. The vertical bars represent the amount of force measured by each of the areas of the force plate. The solid horizontal lines represent the range of vertical force measured to ensure loading of body weight on the lower extremities and not through the arms if participants needed to steady themselves with the provided hand support. If the participant's body weight was shifted to one side more than 5%, the vertical bars changed colors to inform the participant to lean toward the side that was unloaded, as shown in (B). If the participant loaded/unloaded more than +/- 5% of their body weight off their legs, the background screen color would change as shown in (C). Please click here to view a larger version of this figure.
5. Standing corticomotor response assessment
- Begin the neurophysiological assessments by identifying a stimulator intensity that produces consistent motor evoked potentials (MEP), i.e., EMG signal amplitude > 50 µV, and/or a visible corticosilent period in the active muscles, in the target TA, and SOL muscle.
NOTE: Use a double-cone coil to deliver all TMS pulses with the current moving through the coil in an anterior to posterior direction. Apply the TMS pulses only when the participant is maintaining equal weight distribution between their paretic and non-paretic legs, as indicated by the visual feedback/bar graphs mentioned in the previous section (section 4.2).- Test the paretic limb first by applying TMS pulses to the lesioned hemisphere. Begin by setting the TMS stimulator power level to 50% maximal stimulator output (%MSO) by turning the output control knob. Apply a single pulse at 50% MSO to the middle grid point located just lateral to the longitudinal fissure by pressing the trigger button on the stimulator. Apply 2-3 pulses with an interstimulus interval of 5-10 s.
NOTE: If a participant shows a response at 50% MSO, skip to section 5.2 and begin hotspot identification. - If responses are not seen in the TA and SOL, increase the stimulator power by 10% MSO by turning the output control knob and deliver 2-3 TMS pulses as in step 5.1.1.
- If no responses are seen after increasing the stimulator to 60% MSO, again increase the power by 10% MSO. If no MEPs are elicited at 70% MSO, randomly select several grid points and apply TMS pulses to determine whether there is a response at the current power setting.
- If no responses are recorded at any grid point at the current 70% MSO, return to the initial target grid point land, continue to increase the stimulator power by increments of 10% MSO and apply 2-3 stimulations as previously described.
NOTE: Repeat this process until reliable responses are recorded from the target muscles or until it is determined that the participant has no response to TMS. Not all participants will produce a measurable response to TMS.
- Test the paretic limb first by applying TMS pulses to the lesioned hemisphere. Begin by setting the TMS stimulator power level to 50% maximal stimulator output (%MSO) by turning the output control knob. Apply a single pulse at 50% MSO to the middle grid point located just lateral to the longitudinal fissure by pressing the trigger button on the stimulator. Apply 2-3 pulses with an interstimulus interval of 5-10 s.
- Once the stimulator power that produces a consistent response has been identified, begin identifying the hotspot, i.e., the scalp location that produces the largest response to the applied TMS pulses.
- Start a new hotspot trial by clicking Start and selecting Hotspot. Apply a single-pulse stimulation to each of the 15 grid points at the suprathreshold power level identified in the previous steps. Using the image guidance system, move the coil to the first grid point.
- Once the coil is in the proper position, apply the TMS pulse by pressing the trigger button on the stimulator unit. Next, move the coil to the next grid location and apply another single TMS pulse. Continue until a single stimulation has been applied to each grid point and click on Stop to end the trial.
- Examine the amplitudes of the sEMG signals recorded at each grid point. Visually identify the grid points with the largest MEP amplitude, recorded in the sEMG signals, for each of the targeted muscles. The grid locations with the largest MEP amplitudes are the hotspots and will be used to measure the corticomotor response in the following sections.
NOTE: On some occasions, a single grid location may provide the largest MEP amplitudes for both the TA and SOL. In these cases, determine the motor thresholds for each muscle separately.
- Next, determine the motor threshold of the targeted muscle using simple adaptive Parameter Estimation by Sequential Testing (PEST)19,20.
- Open the PEST program and set the initial stimulator intensity to the suprathreshold value used to identify the hotspot by typing the value into the box.
- Begin a new PEST trial by clicking the Start tab in the data collection software and select PEST.
- Apply a single TMS pulse to the identified target muscle's hotspot at the initial %MSO intensity displayed in the PEST program. Indicate in the PEST program that a response was observed in the muscle's sEMG signal by typing y or n. The PEST program will automatically calculate the next stimulation intensity.
- Adjust the stimulator's power level to match the PEST program and apply another single TMS pulse. Continue this process until the PEST program determines the motor threshold, indicated by a change in color of the stimulation intensity, and end the data collection trial by clicking on the Stop tab.
NOTE: The PEST procedure uses a freely available program that directs how much stimulator power to use with successive pulses. One of the PEST programs can be found here: (https://www.clinicalresearcher.org/software.htm).
- After the target muscle's hotspot and motor threshold have been identified, begin the CMR evaluation. Set the intensity of the stimulator to 120% of the determined motor threshold.
- Initiate a new trial in the data collection software by clicking on the Start tab and select an MEP trial. Place the coil on the muscle's hotspot and apply 10-20 single-pulse stimulations.
- Allow for 5-10 s between each stimulation. Record the evoked sEMG responses for off-line analysis. Allow the participant to rest ad libitum and for sufficient time between testing procedures to reduce the likelihood of the participant developing fatigue, which could affect the results.
- Click on the Stop tab after recording the MEPs to end the trial.
NOTE: The researcher handling the TMS coil should ensure that the participants have equal weight distribution under each leg immediately prior to applying any TMS pulse. If the investigator thinks the stimulation was applied while the participant's weight was not equally distributed, perform an additional stimulation and exclude the previous trial from future analysis. Test the non-paretic muscles immediately after the paretic muscles. Figure 2 displays the experimental setup during the standing TMS assessment.
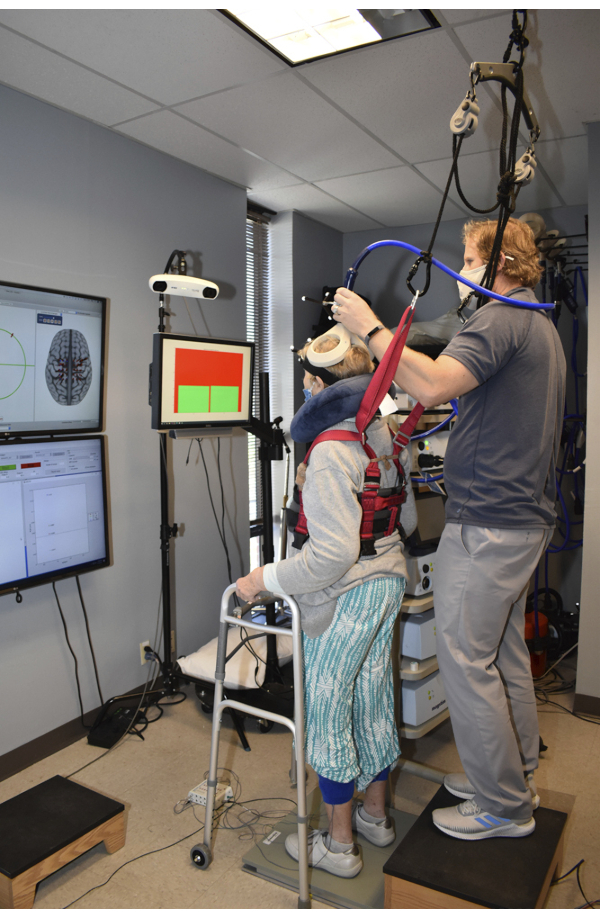
Figure 2: Image taken during the measurement of the corticomotor response (CMR) in the standing position. The image guidance system and the collected sEMG activity are displayed to research personnel during data collection as shown on the monitors located on the left side of the image. Visual feedback of the weight distribution was provided in front and slightly to the right of the participants. Participants wore a safety harness which was attached to the ceiling to prevent falls while standing on the dual-top force plate. Support for the participants' arms was provided to help participants steady themselves after TMS pulses were applied. Please click here to view a larger version of this figure.
6. Sitting corticomotor response assessment
- After the completion of the standing TMS assessment, remeasure the motor thresholds and the CMR in a resting/sitting position.
- Use the same procedures previously described (sections 5.2-5.4). The only change being the participant should be seated in a chair with their legs supported and muscles relaxed.
- Use the same hotspots identified during the standing assessment (section 5.2) in the sitting position. Perform the neurophysiological testing in the same manner as used in the standing position, except for using a stimulation intensity of 120% of the resting/sitting motor threshold.
NOTE: It may be necessary to perform additional testing using a previously determined stimulator power. For example, if comparisons between the amplitude of the MEP in different postural positions are performed, it may be necessary to use a similar absolute stimulator power. This will depend upon the research question at hand and should be identified during study design.
7. Statistical approach
- To test the hypothesis that standing would lead to an increased probability of evoking measurable responses construct a 2 x 2 table and test the proportions using McNemar's Test21.
- To compare the power levels of the motor thresholds, use a paired t-test on the participants who had measurable responses in both positions. Determine significance with an alpha = 0.05.
One participant was removed from the analysis due to the inability to tolerate the standing TMS procedure due to preexisting knee pain and a diabetic wound received before their arrival to the research laboratory, leaving a final sample size of 15. The diabetic wound was directly over the TA and precluded any sEMG measures of this muscle. There were no major adverse events reported to the investigators during either the sitting or standing TMS procedures. Several minor adverse events were reported, such as neck muscle pain and slight headaches. However, these minor events were reported at the end of the testing session, and it was not clear whether the sitting or standing procedures were more responsible for these side-effects. These minor adverse events are commonly seen after TMS evaluations and within the TMS literature22.
Total loading/unloading of body weight during TMS pulse application was +0.4% (SD 1.8%) of body weight. This signifies that the participants did not unload body weight from their legs to their arms when using the rollator as a means to support themselves during the TMS procedures. The average weight distribution of the participants' left leg was 50% (SD 6%). We attempted to measure motor thresholds in four separate muscles (paretic and non-paretic, TA and SOL), leading to a total of 60 motor thresholds in both the standing and sitting positions. In the standing position, we were able to elicit and measure a motor threshold 90.0% of the time compared to 65.0% in the sitting position. Within a single session, it was more likely that assessing the motor threshold in the standing position would result in a measurable response (McNemar Chi2, Yates correction, χ = 8.48, P = 0.004) (Table 2). This agrees with our first hypothesis that the standing position would result in an increased likelihood of evoking measurable responses. Our second hypothesis was that standing would result in motor thresholds requiring lower stimulator power. Our results show that when individuals presented with measurable motor thresholds in the sitting and standing positions, the measured thresholds in the standing position were lower (N = 38, Standing MT 45% MSO SD 9, Sitting MT 53% MSO SD 11, Paired t-statistic 4.99, P < 0.001). Figure 3 displays the measured motor thresholds for each muscle and condition for all participants.
| Sitting Response |
Standing Response | ||||
| Yes | No | Total | % | ||
| Yes | 38 | 1 | 39 | 65 | |
| No | 16 | 5 | 21 | 35 | |
| Total | 54 | 6 | 60 | ||
| % | 90 | 10 | 100 | ||
Table 2: The constructed 2 x 2 table shows the reported ability to successfully produce a response to TMS and the ability to measure a motor threshold in the sitting and standing conditions. The McNemar's test was used to compare the probability of eliciting a measurable response and it was found that the standing assessments were significantly more likely to evoke a measurable response compared to performing evaluations in a sitting position.
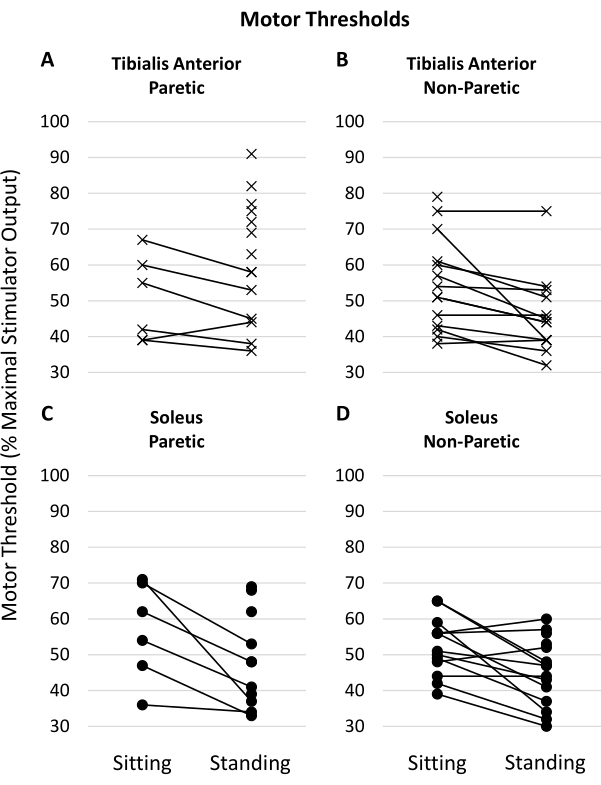
Figure 3: Measured motor thresholds in the muscles of interest. Lines connecting the left and right values indicate the individual had measurable motor thresholds for that muscle in both the sitting and standing positions. Motor thresholds are measured and reported as a percentage of maximal stimulator output (%MSO). (A,B) show motor thresholds measured in the paretic and non-paretic tibialis anterior muscles, respectively. (C, D) show the motor thresholds of the paretic and non-paretic soleus muscles, respectively. Please click here to view a larger version of this figure.
