Mechanical and thermal QST has been performed to detect sensory thresholds in both research and client-owned dogs under various clinical conditions, including normal, healthy dogs, dogs with chronically painful conditions such as OA, dogs with acute spinal cord injury, and to assess post-operative pain and effectiveness of analgesics. Though there is a growing body of work on QST in dogs, no normal range of values has been established for any testing modalities. However, several studies have assessed the feasibility and repeatability of mechanical and thermal QST in dogs, showing QST data as accurate measurements of sensory thresholds in dogs8,9,15,16.
The values reported here are from a previously published data set of 23 normal dogs who were older than 2 years of age, weighed greater than 15 kg, had no abnormalities detected on orthopedic and neurologic examination, and had no history of impairment reported by the owner10. This group of dogs included 8 mixed breed dogs, 4 Labrador retrievers, 6 golden retrievers, and 1 each of: American Staffordshire terrier, Australian cattle dog, otterhound, Australian shepherd dog, and German shorthaired pointer. Mechanical and hot thermal QST data from these dogs, which represent typical data obtained for QST in dogs, are summarized in Table 3 and graphically represented in Figure 4, Figure 5, and Figure 6. To obtain the average QST value for each modality in each dog, based on previous work and analysis of the replicate effect16, we recommend that the dog's highest and lowest values from the five trials of the QST modality are eliminated, and the remaining three values are averaged. The original study used a repeated-measures mixed-effects models to determine the influence of covariates, including age, sex, body weight, and feasibility score. Then, the association between covariates and the QST threshold was evaluated using Wald tests10. This analysis showed no significant effect of age, sex, and feasibility score on the values of any of the QST modalities (p > 0.05) and a substantial impact of body weight on the values of hot thermal QST (p = 0.006), but neither of the other two modalities. There were not enough dogs of any breed to assess the effect of breed on the QST values.
When interpreting mechanical and thermal QST data, lower pressure thresholds and shorter latency times indicate greater sensitivity to the applied stimulus, while higher pressure thresholds and longer latency times indicate less sensitivity. A variety of clinical conditions have been shown to affect sensory thresholds in dogs. Though there is some inconsistency in the data, most studies report lower sensory thresholds (greater sensitivity, hyperalgesia) in dogs with OA both at the primary site of the joint(s) affected by OA and at secondary sites distant to the affected joint(s)8,9,10. All studies that have assessed sensory thresholds in dogs with acute thoracolumbar spinal cord injury report higher sensory thresholds (decreased sensitivity, hypoalgesia) in the pelvic limbs of these dogs3,4,5. Studies assessing post-operative pain in dogs undergoing ovariohysterectomy have indicated lower sensory thresholds at the surgical site and at a distant secondary site in the pelvic limbs (distal tibia) that were alleviated by pre-and post-operative administration of analgesic medications11,12. Thus, the population of dogs being assessed and their medical history, including the chronicity of pain and administration of analgesic medications, should be considered when determining expected results and interpreting data.
Feasibility scores are used to indicate the ease with which QST data were obtained from each subject for each testing modality. Feasibility scores are assigned based on a 6-point scale (0-5). They are determined based on the dog's level of cooperation with testing, the amount of restraint needed to accomplish testing, and the clarity of the dog's reaction to the applied stimuli (Table 1). Increasing scores on the feasibility scale indicate the increasing difficulty of data collection, with scores of 0-2 considered easy data collection and 3-5 considered difficult data collection. Mechanical and hot thermal QST is generally well-tolerated in dogs. Studies have reported feasibility scores to show that most dogs have feasibility scores indicating easy data collection8,10,15. Feasibility scores also indicate the quality of data collected, as dogs who require significant restraint, are not cooperative, are sensitive to their feet being touched, or who have unclear or inconsistent reactions to the applied stimuli decrease the QST operator's confidence that the data collected truly represent the dog's sensory thresholds (versus being an indication of the dog's reaction to these factors).
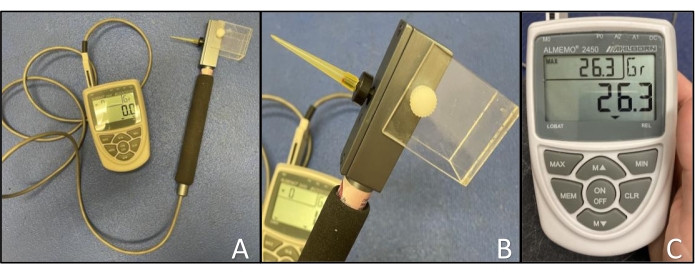
Figure 1: Electronic von Frey anesthesiometer. (A) Device set-up showing the rigid von Frey tip applied to the load cell and the cord from the handpiece connected to the recording device through the M0 channel. (B) Close-up of the von Frey tip attached to the load cell. (C) Close-up of the recording device showing the arrangement of buttons and displaying the current force (center), maximum force (upper left), and units (upper right). Please click here to view a larger version of this figure.
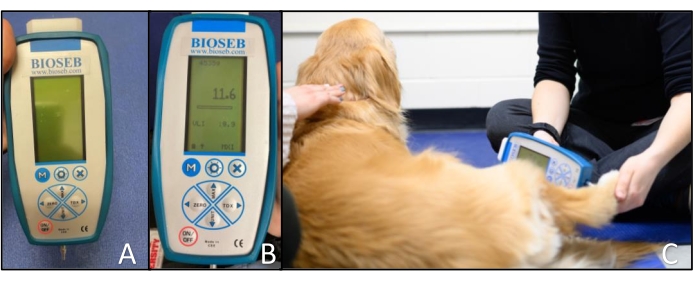
Figure 2: Blunt probed pressure algometer. (A) Device set-up showing the small blunt probe attached to the recording device. (B) Close-up of the recording device showing the arrangement of buttons and displaying the maximum force (center) and units (top). (C) Application of the blunt probed pressure algometer to the dorsal metatarsal region of a dog. The tip is applied perpendicular to the skin. Please click here to view a larger version of this figure.
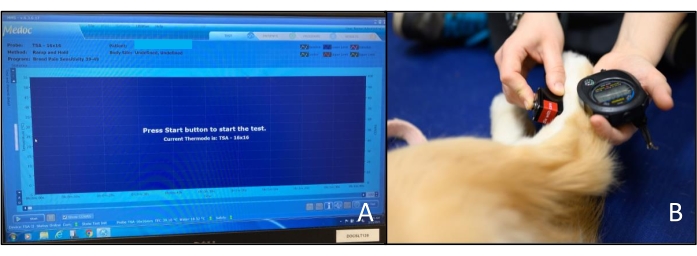
Figure 3: Hot thermosensory analyzer. (A) Computer screen display when the analyzer is ready to start a test. The Start button is in the lower-left corner of the screen. (B) Application of the thermode to the dorsal metatarsal region of a dog. The QST operator also operates the stopwatch with the hand supporting the limb. Please click here to view a larger version of this figure.
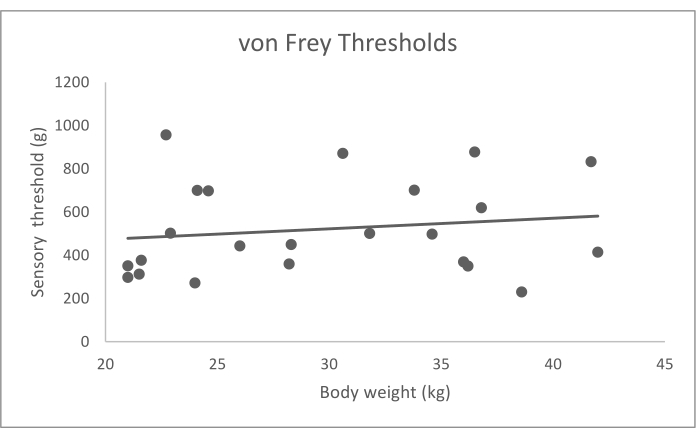
Figure 4: Electronic von Frey anesthesiometer sensory thresholds (g) data by body weight (kg). Bodyweight did not have a significant effect on sensory thresholds (p = 0.905). Please click here to view a larger version of this figure.
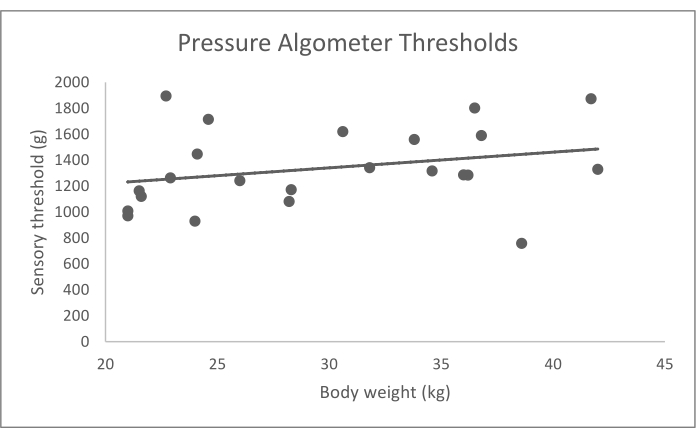
Figure 5: Data for blunt probed pressure algometer sensory thresholds (g) by body weight (kg). Bodyweight did not have a significant effect on sensory thresholds (p = 0.734). Please click here to view a larger version of this figure.
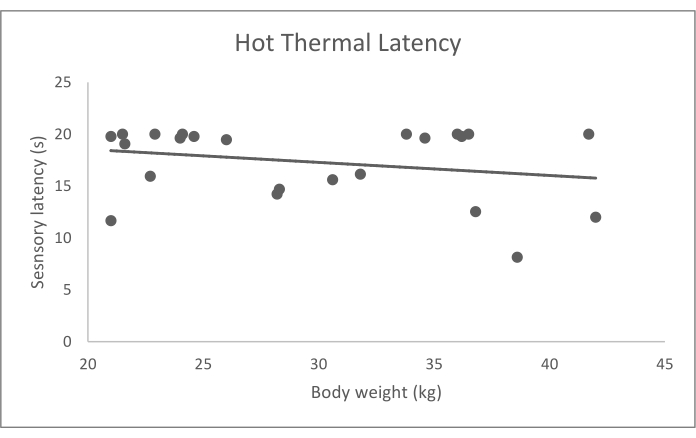
Figure 6: Hot thermal probe sensory latency (s) data by body weight (kg). Bodyweight had a significant effect on sensory latency (p = 0.006). Please click here to view a larger version of this figure.
| Feasibility score | Description | |
| 0 – No problem | Minimum restraint needed; excellent cooperation; clear reaction to stimuli | |
| 1 – Mild difficulty | Mild restraint needed; good cooperation; clear reaction to stimuli | |
| 2 – Moderate difficulty | Moderate restraint needed; good cooperation > 50% of the time; mild sensitivity of feet being touched; mild variation in reaction to stimuli | |
| 3 – Significant difficulty | Significant restraint needed and resisted lateral recumbency; good cooperation < 25% of the time; moderate sensitivity to feet being touched; moderate variation in reaction to stimuli | |
| 4 – Extreme difficulty | Constant restraint required; not cooperative; unclear reaction to stimuli, not confident in data collected |
|
| 5 – Impossible | Could not collect data due to the dog's disposition and/or lack of confidence in the reactions seen being due to the stimulus | |
Table 1: QST feasibility scoring rubric. Rubric used for evaluation of the ease with which mechanical and thermal QST data can be collected from dogs. Feasibility scores range from 0 = no problem to 5 = impossible.
| Parameters | Input |
| Method | Ramp and hold |
| Sequence | 1 |
| Baseline | 39 |
| Time Before Sequence (s) | 0 |
| Trigger | Auto |
| Destination Temperature (°C) | 49 |
| Deatinaytion Rate | 8 |
| Destination criterion | Temperature |
| Duration time (s) | 30 |
| Return option | Baseline |
| Return Rate | 1 |
| Number of Trials | 1 |
Table 2: Program details for the hot thermal probe.
| Average ± SD | Range | |
| Electronic von Frey (g) | 521.1 ± 216.8 | 230.2 – 957.1 |
| Pressure algometer (g) | 1338.0 ± 308.6 | 758.9 – 1894.0 |
| Hot thermal probe (s) | 17.31 ± 3.55 | 8.13 – 20 |
Table 3: Average and range of values of mechanical and hot thermal QST results in 23 normal dogs. The highest and lowest values of the five trials from each modality were excluded, and then the values of the remaining three trials were averaged for each dog. The overall average, standard deviation, and range were calculated from these individual averages. Thresholds for the von Frey and pressure algometer are reported in grams (g), and latency for the hot thermode is reported in seconds (s). All measurements were taken at the dorsal metatarsal region.
