This protocol demonstrates the induction of uveitis in mice using the primed mycobacterial uveitis model (PMU). Ensuring consistency in the subcutaneous injection and accuracy of the intravitreal injection are key steps in developing the primed mycobacterial uveitis model (PMU). Figure 1 demonstrates the mouse intravitreal injection procedure using a stereotaxic apparatus. Ear bars help to gently position the head in the same location under the microscope (Figure 1E). They also keep the head stable during the intravitreal injection procedure, which decreases the risk of injection trauma. Following a successful injection, fluorescein in the injection solution produces a greenish reflection from within the eye that can be seen under the microscope or from a side view as pictured in Figure 1F.
When performed as outlined, the protocol generates robust acute uveitis that can be detected using OCT and fundus imaging as early as 10 h after intravitreal injection. Figure 2 demonstrates the correct alignment of the eye for OCT imaging. Table 1A lists the parameters used in the OCT protocol. A systematic approach to obtaining images will provide high-quality images that can be compared over time. Anterior chamber images are centered on the apex of the cornea using the en face SLO image (Figure 2A) with the iris aligned in parallel to both the horizontal and vertical planes (Figure 2B,C). Volume and line scans are captured with a vertical alignment such that inferior and superior regions can be viewed simultaneously. Posterior segment images are centered on the optic nerve using the en face SLO image (Figure 2D), and the bright band of the RPE is used to align the retina in parallel to both the horizontal and vertical planes (Figure 2E,F).
Figure 3 shows typical findings of PMU ocular inflammation using OCT imaging. Twenty four hours after intravitreal injection, inflammatory cells are seen in the aqueous and vitreous (Figure 3B). In the presence of moderate or severe inflammation, a hypopyon will be seen in the inferior angle in the AC. The degree of ocular inflammation can be scored on these OCT images using the criteria listed in Table 2. Representative examples of images demonstrating the inflammatory features typical for each score are shown in Figure 4. AC and PC chamber scores can be added together to generate the combined OCT score. Combined scores >0 but ≤2.5 represent mild inflammation. Moderate inflammation is determined by scores >2.5 but ≤4.5. Scores >4.5 identify severe inflammation. Inflammation typically peaks 48 h after intravitreal injection with OCT scores in the AC and PC between 1 and 3 (combined scores between 2 and 6). AC and PC scores of 0.5 or 4 are less common. In the case scores outside the typical range are encountered frequently, troubleshooting may be required to identify the factors contributing to outlier scores (see discussion section). Inflammation scores in the anterior chamber tend to return to zero within one week following intravitreal injection. In contrast, posterior scores do not return to zero; instead, low-level chronic inflammation persists in the form of vitritis, and perivascular lymphocytes infiltrate in the retina for 1-2 months following intravitreal injection.
Inflammation score in PMU can also be determined using histology. Figure 5 shows representative H&E sections for use in scoring the severity of PMU by histology. The number of inflammatory cells in the aqueous and vitreous are counted and used to determine the severity using the score criteria listed in Table 3. Inflammatory cell infiltration of the ciliary body is commonly seen on one side of the histology section (unilateral involvement) in mild or moderate inflammation. When inflammation is severe, this is reflected by the presence of an inflammatory cell infiltrate in the ciliary body on both sides of the lens (termed bilateral involvement). During later time points after intravitreal injection, chronic inflammation manifestations, including the presence of perivascular and intraretinal leukocytes and outer retinal folds, can also be identified. Histology can also be helpful in identifying eyes impacted by poor injection techniques. Trauma to the lens during the intravitreal injection can be identified by the presence of amorphous eosin-stained (pink) lens proteins outside the lens capsule adjacent to the area of trauma. Reflux of the intravitreal mTB into the subconjunctival space will generate inflammation outside the eye that can be identified by a careful review of periocular structures present on the sections. Due to the failure to retain mTB extract within the eyes, these eyes will typically have low OCT scores of inflammation.
Brightfield fundus imaging can also be used to identify clinically relevant aspects of PMU, including the development of a hypopyon, vitritis, and retinal or perivascular inflammatory cell infiltration. Figure 6 shows two examples where retinal and perivascular inflammation can be seen on fundus images. These two eyes also show the range of inflammation that is common in the PMU model. Table 1B lists the parameters used in the fundus/retinal OCT imaging system. Note the impact that severe inflammation has on the image quality (Figure 6, day 2, OCT and fundus images in the top row) and the extent of disease present on day 21. Corneal edema can also decrease image quality during acute inflammation; however, it is uncommon for corneal edema to be severe from inflammation alone. More commonly, the image quality will be degraded by epithelial damage resulting from incomplete surface protection during imaging and anesthesia events.
The PMU model can be used to induce uveitis in any mouse breed or genotype. In albino eyes, OCT can still be used to score inflammation, but the absence of fundus pigment makes visualization of inflammation challenging by brightfield imaging13,34. Post mortem studies can be performed on ocular tissues, regional lymph nodes, or the spleen. Some examples include assays for the presence of immune cells such as flow cytometry and immunohistochemistry and measurement of inflammatory cytokines. At all time points tested after initiation of inflammation with PMU (day 1 to day 56), there are sufficient CD45+ inflammatory cells present in individual eyes to detect many major leukocyte populations in the eye by multi-parameter flow analysis12,35. Aqueous (2-5 µL) and vitreous (5-10 µL) humors can be collected from inflamed eyes for protein concentration determination, proteomic studies, or cytokine concentration determination36.
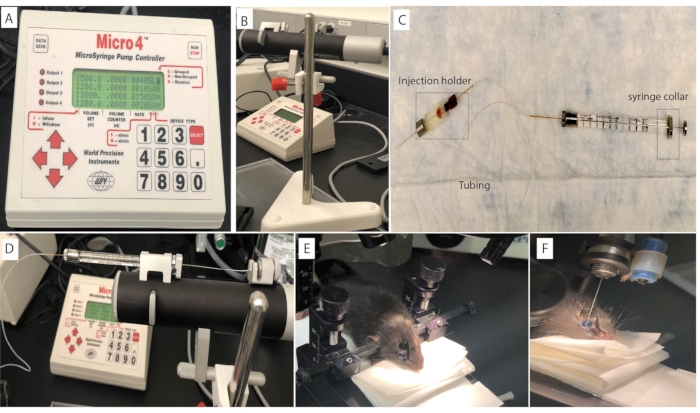
Figure 1: Mouse intravitreal injection set up. The intravitreal injection is performed on the mouse eye using (A) a microsyringe pump controller connected to the (B) Micropump and (C) an injection syringe. The syringe is loaded and mounted on the (D) Micropump. The mouse head is positioned using (E) ear bars to ensure stability and consistency during the intravitreal injection procedure. (F) Fluorescein in the injection solution produces a greenish reflection from within the eye after a successful procedure. Please click here to view a larger version of this figure.
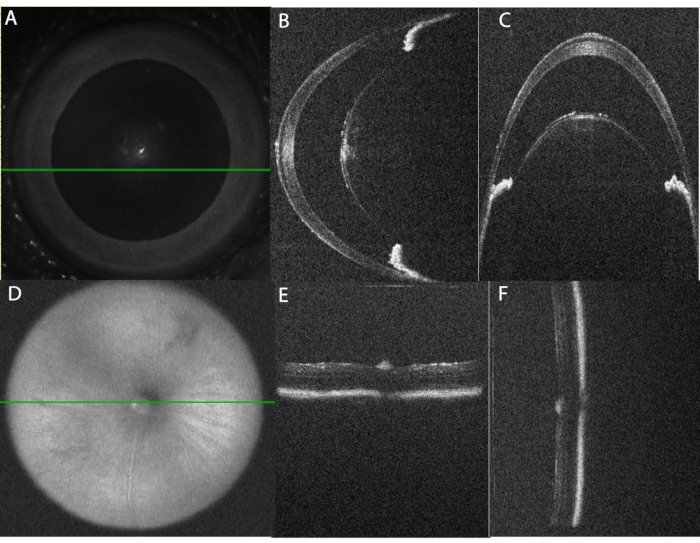
Figure 2: Proper alignment of the eye for OCT imaging. (A) Using the en-face scanning laser ophthalmoscope (SLO) image, the eye is centered for anterior chamber imaging. The green line indicates the position of the horizontal line scan shown in panel (B). Note that the central cornea is avoided to decrease reflection artifact. (C) Vertical B-Scan through the paracentral anterior chamber. This scan is obtained at 90° from the horizontal scan. Note that the alignment of the iris sections on each side of the lens is level in the horizontal scan (panel B) and arranged one above the other in the vertical scan (panel C). (D) Using the SLO image, the posterior chamber image is centered on the optic nerve. (E) Horizontal B-Scan Alignment, (F) Vertical B-Scan Alignment. Please click here to view a larger version of this figure.
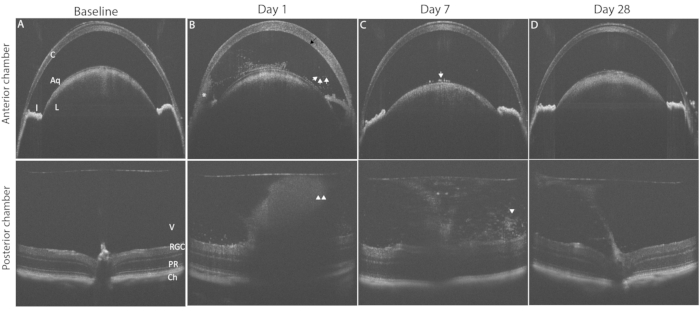
Figure 3: Induction of PMU generates panuveitis that can be monitored by longitudinal OCT imaging. The top row shows anterior chamber (AC); the bottom row shows posterior chamber (PC) OCT images to highlight pathological changes in the disease course. (A) Baseline OCT image of the AC (top) and PC (bottom) prior to induction of uveitis, both score 0. (B) Day 1 after intravitreal injection showing the presence of corneal edema (black arrow), a hypopyon (*) multiple free-floating inflammatory cells in the AC (white arrows), and vitritis (white arrowheads) in the PC. (C) Day 7 after intravitreal injection with few AC cells on the anterior lens capsule (white arrow) and decreased vitritis (white arrowhead). (D) Day 28 after intravitreal injection anterior chamber with resolved AC inflammation and mild vitritis. Abbreviations: C- cornea, L – lens, I – iris, Aq – aqueous, V vitreous, RGC – retinal ganglion cells, PR – photoreceptors, Ch- choroid. Please click here to view a larger version of this figure.
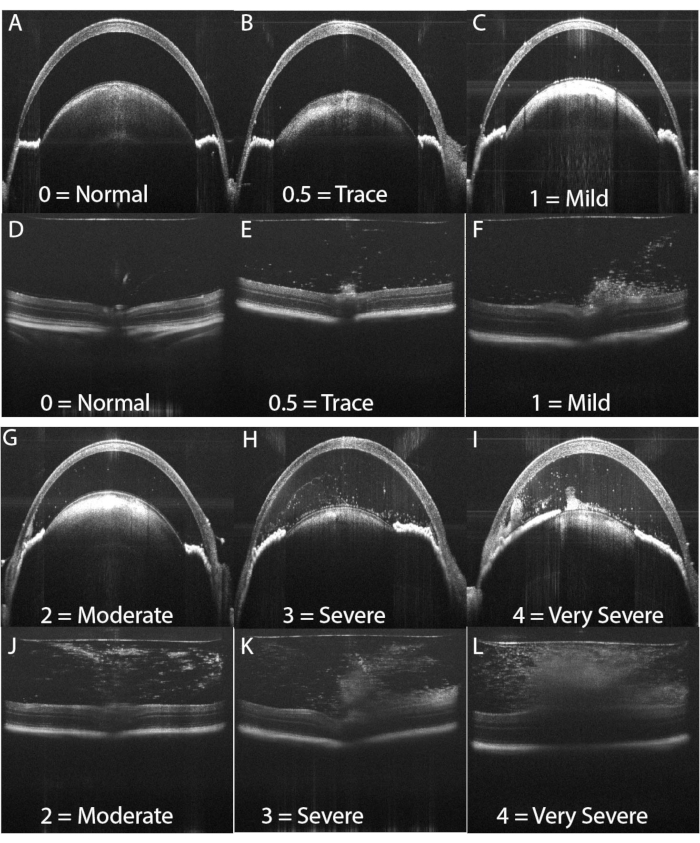
Figure 4: OCT score examples. An OCT score between 0 and 4 is assigned to each AC image and PC image using the categorical system shown in Table 2. The AC and PC scores are combined for the final OCT score for the eye. (A,D) Examples of a score of zero. (B,E) Examples of a score of 0.5. (C,F) Examples of a score of 1. (G,J) Examples of a score of 2. (H,K) Examples of a score of 3. (I,L) Examples of a score of 4 are shown in panels I and L. Please click here to view a larger version of this figure.
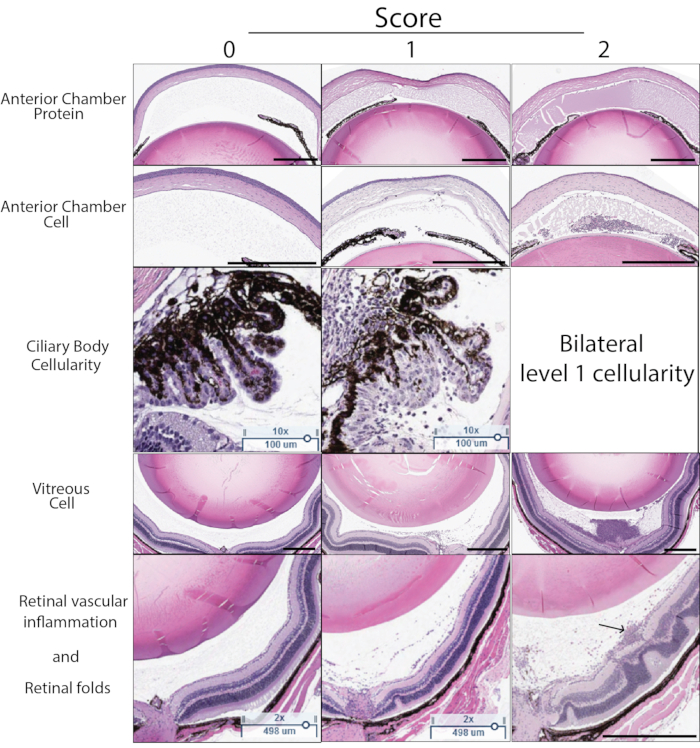
Figure 5: Histology score examples. Histology score is determined based on five characteristics visible in H&E sections: Anterior chamber protein density, anterior chamber cell number, immune cell infiltration of the ciliary body, vitreous cell density, retinal vascular inflammation, and structural retinal changes. A score of 0-2 is assigned for each characteristic. The description of each score is found in Table 3. A representative example score of 0-2 for each characteristic is shown in this figure. The left column demonstrates the score of zero. The center column shows examples of score 1. The right column shows examples of score 2. A score of 2 for ciliary body score is assigned if the ciliary body on either side of the lens in the same section demonstrates cellular inflammation. The final histology score is the sum of the score for each of the five criteria (max score 10). The arrow in the bottom right panel indicates perivascular leukocytes associated with a superficial retinal vessel. Black scale bar indicates 500 µm. Ciliary scale bars indicate 100 µm. Please click here to view a larger version of this figure.
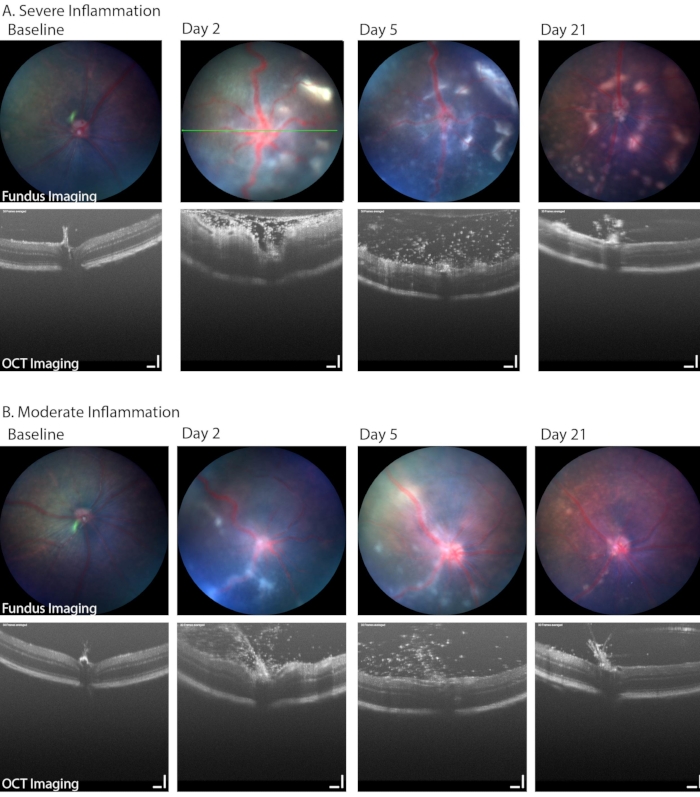
Figure 6: Longitudinal fundus imaging in PMU identified a range of disease severity. (A) Severely inflamed eyes demonstrate multiple white infiltrates in the retina and vascular tortuosity on color fundus imaging (top row) as well as dense vitritis and retinal edema on OCT (bottom row) on day 2. Progression in the number of retinal lesions can be seen over time while the vitritis improves. Green line indicates the position of the OCT image. (B) Mildly inflamed eyes demonstrate fewer and more discrete linear lesions in the fundus and a number of infiltrating cells in the vitreous space. Scale bar = 100 µm. Please click here to view a larger version of this figure.
| A | |||
| Mouse Anterior Chamber | Fast Scan | Volume Scan | Linear Scan |
| Length X Width | 4.0 mm x 4.0 mm | 3.6 mm x 3.6 mm | 3.6 mm |
| Angle | 0 | 90 | 90 |
| A-scan/B-Scan | 800 | 1000 | 1000 |
| # B-scans | 50 | 400 | 1 |
| Frames/ B-scan | 1 | 3 | 20 |
| Mouse Posterior Chamber | Fast Scan | Volume Scan | Linear Scan |
| Length X Width | 1.6 mm x 1.6 mm | 1.6 mm x 1.6 mm | 1.6 mm |
| Angle | 0 | 0 | 0 |
| A-scan/B-Scan | 800 | 1000 | 1000 |
| # B-scans | 50 | 200 | 1 |
| Frames/ B-scan | 1 | 3 | 20 |
| B | |||
| Mouse Posterior Chamber | Volume Scan | Linear Scan | |
| Length X Width | 0.9 mm x 0.9 mm | 1.8 mm | |
| Angle | 0 | Any (typically 0 or 90) | |
| A-scan/B-Scan | 1024 | 1024 | |
| # B-scans | 512 | 1 | |
| Frames/ B-scan | 1 | 30 |
Table 1: Scan parameters. (A) OCT scan parameters. (B) Fundus/retinal OCT scan parameters
| OCT Score descriptions | ||||||
| Score | Anterior Chamber | Posterior Chamber | ||||
| NA | No view beyond anterior cornea | No view of posterior segment | ||||
| 0 | No inflammation | No inflammation | ||||
| 0.5 | 1–5 cells in the aqueous | Few cells occupying less than 10% of the vitreous area | ||||
| OR corneal edema | No subretinal or intraretinal infiltrates or retinal architecture disruption | |||||
| 1 | 6–20 cells in the aqueous | Diffuse cells (no dense clumps) occupying between 10 and 50% of the vitreous area. | ||||
| OR a single layer of cells on the anterior lens capsule | No subretinal or intraretinal infiltrates or retinal architecture disruption | |||||
| 2 | 20–100 cells in the aqueous | Diffuse cells (no dense clumps) occupying > 50% of the vitreous area | ||||
| OR fewer than 20 cells and a hypopyon present | No subretinal or intraretinal infiltrates or retinal architecture disruption | |||||
| 3 | 20–100 cells in the aqueous | Diffuse cells equal to grade 2 and 1 | ||||
| AND a hypopyon OR a pupillary membrane | AND at least one dense vitreous opacity occupying 10%–20% of the vitreous area OR the presence of vitreous cells equal to grade 2 and rare (≤ 2) subretinal or ntraretinal opacities | |||||
| 4 | Any number of aqueous cells | Dense vitreous opacity occupying > 20% of the vitreous area. | ||||
| AND a large hypopyon and pupillary membrane OR anterior structure loss due to severe inflammation | OR diffuse vitreous cells with large subretinal or intraretinal opacities | |||||
Table 2: PMU OCT score criteria: OCT images are scored according to the criteria listed in the table. AC and PC scores are added to obtain the final score of the eye. In cases where a clear view of the eye was not acquired, a score of NA was assigned to the images, and these were excluded from the study.
| Histology Score Description | |||
| Characteristic | 0 | 1 | 2 |
| Anterior Chamber (AC) Protein | Scant acellular particles staining with eosin in the AC | Moderate, but not confluent, extracellular eosin staining anywhere in the AC | Confluent or near confluent extracellular eosin staining throughout the AC |
| Anterior Chamber (AC) Cell | No cells | 1–100 cells, but no dense aggregations of cells | >100 cells, or dense aggregations of cells |
| Ciliary Body Inflammation | No leukocyte infiltration of the ciliary body or surrounding vitreous | Unilateral presence of leukocytes infiltrating the ciliary body and/or the surrounding vitreous. | Bilateral presence of leukocytes infiltrating the ciliary body and/or the surrounding vitreous. |
| Retinal Vascular Inflammation | No retinal vessels with perivascular leukocytes | One vessel per section with perivascular leukocytes | >1 vessel per section with perivascular leukocytes |
| Retinal fold or damage | No retinal damage | 1–3 retinal folds per section | >3 retinal folds per section, or any other retinal layer destruction or intraretinal hemorrhage |
Table 3: PMU histology score criteria: H&E sections of the eye were scored based on the criteria listed in the table. Three sections from the same eye were scored and averaged to obtain the final histology score of the eye.
