The GRIN lens-based in situ imaging modality can allow visualization of the tracheal inner lumen in situ (Figure 5A). Using this imaging method, both bright-field and fluorescent images of the native and de-epithelialized tracheas can be obtained (Figure 5B,C). No fluorescent signal was observed from the native trachea prior to CFSE labeling (Figure 5Bii). However, when the tracheal epithelium was labeled with CFSE dye, a uniform fluorescent signal (green) was observed throughout the epithelium (Figure 5Ci). Following de-epithelialization via SDS and vibration-assisted airway irrigation, the intensity of the fluorescent signal was decreased significantly (Figure 5Cii), indicating ablation of the epithelium.
The H&E images of de-epithelialized trachea showed the removal of the pseudostratified epithelium from the trachea lumen and preservation of the cells and ECM microstructure in underlying tissue layers (Figure 6A). Moreover, pentachrome (Figure 6B) and trichrome staining (Figure 6C) confirmed the maintenance of the trachea tissue architecture and the ECM components, such as collagen and proteoglycans. Furthermore, immunofluorescence of epithelial cells (epithelial cell adhesion molecule, EpCAM; Figure 6D) and collagen I (Figure 6E) revealed complete removal of the epithelium and preservation of collagen I within the subepithelial tissue. SEM imaging of native trachea showed that the luminal surface of native rat trachea mainly was populated with multi-ciliated cells and goblet cells. On the other hand, SEM images of de-epithelialized trachea lumen showed that the basement membrane was exposed as indicated by a mesh network of ECM fibers and the absence of epithelial cells (Figure 6F).
Using de-epithelialized rat tracheas and fluorescently labeled cells, we investigated whether incorporating a hydrogel as a cell delivery vehicle could achieve homogeneous cell distribution onto the de-epithelialized tracheal lumen (Figure 7A,B). In this study, the mesenchymal stem cells (MSCs) were used as the model cells for the cell delivery and culture study. As described in the protocol (step 5), we instilled MSC-loaded collagen I pre-gel into a de-epithelialized rat trachea and monitored the distribution of the cells on the tracheal lumen using the GRIN lens imaging system. As a control experiment, we suspended MSCs in the culture medium, infused the cell-loaded culture medium into the trachea, and visually inspected the distribution of the cells. In situ imaging results showed that the fluorescently labeled cells delivered via hydrogel remained adhered more uniformly across the lumen than those seeded via culture medium (Figure 7B). We then tested the cell viability before and after cell delivery to evaluate potential cell damage and death due to shearing stress during cell infusion. The result showed that cell viability was not significantly affected by the cell delivery procedure as over 90% of cells remained viable (Figure 7C).
Furthermore, we cultured the cell-seeded tracheas for 4 days. The cells seeded via both collagen and culture medium (control) proliferated on the de-epithelialized trachea lumen surface as indicated by the increased number of cells expressing CFSE over time in both the upper and lower half of the tracheal lumen (Figure 7D). Notably, in the collagen hydrogel delivery group, the difference in the density of the cells between upper and lower lumens was smaller than that in the control group, indicating cell delivery via hydrogel promotes homogeneous cell distribution throughout the trachea lumen.
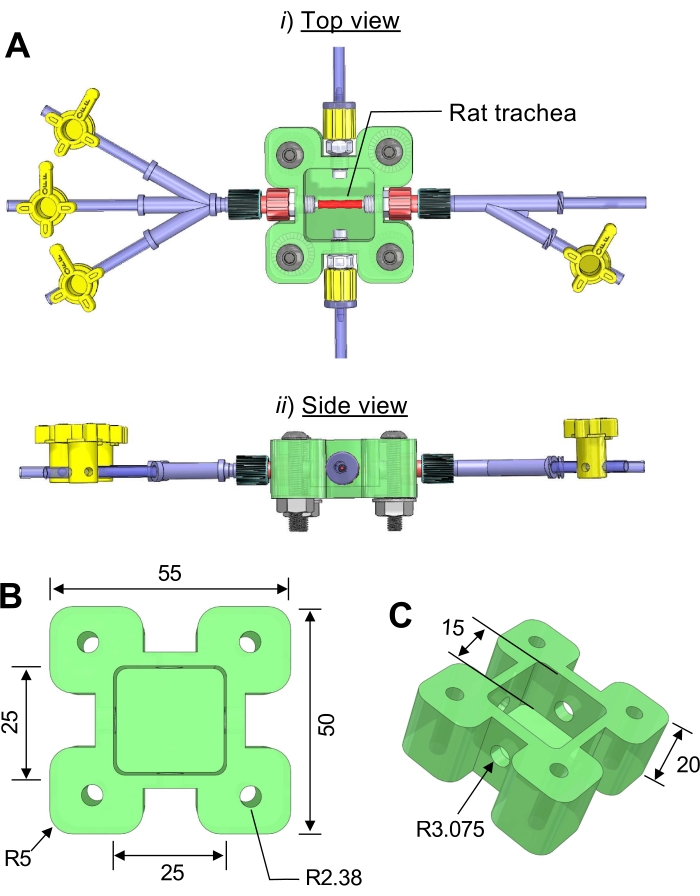
Figure 1: Three-dimensional (3D) computer drawing of the trachea bioreactor. (A) (i) side view, (ii) top view. (B) The dimensions of the bioreactor chamber. (C) A transparent acrylic plastic sheet is cut and attached to the top of the main chamber using screws. Unit = mm; R = radius. Please click here to view a larger version of this figure.
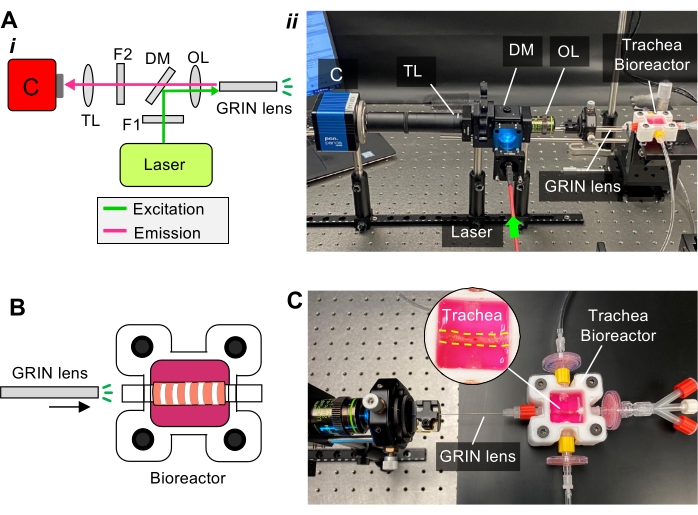
Figure 2: Custom-built micro-fiber imaging for in situ visualization of the rat trachea. (A) (i) Schematic of the imaging setup components of the light path. Abbreviations: C = camera, TL = tube lens, F = filter, DM = dichroic mirror, OL = objective lens; (ii) photograph of the imaging setup components showing the imaging probe (GRIN lens) is inserted in the Luer connector of the bioreactor. (B) Schematic showing that the GRIN lens is integrated with the bioreactor. (C) A photograph showing the imaging probe is used to visualize the trachea inside the bioreactor. Please click here to view a larger version of this figure.
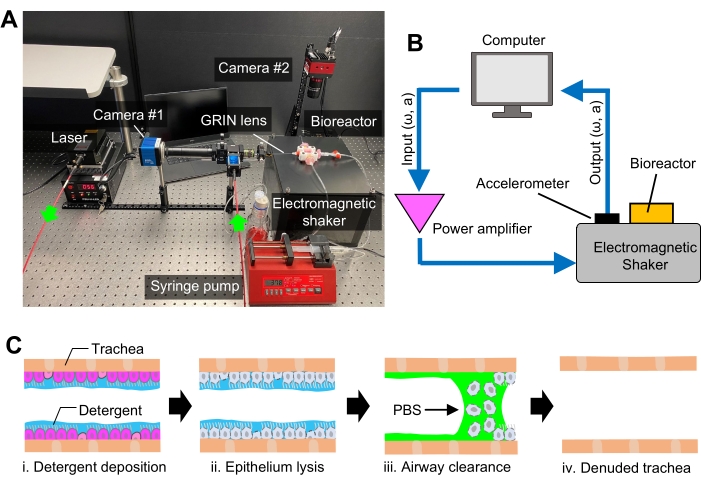
Figure 3: The platform for de-epithelialization of rat trachea. (A) Photograph showing the experimental setup for de-epithelialization and in situ optical fiber imaging. (B) Diagram showing the component and assembly of the custom-built electromagnetic shaker used to facilitate epithelium removal. ω: frequency, a: amplitude (C) Schematic showing the workflow of rat trachea de-epithelialization procedure. PBS = phosphate-buffered saline. Please click here to view a larger version of this figure.

Figure 4: Delivery of exogenous cells into de-epithelialized rat trachea using hydrogel. Schematic showing hydrogel solution used as a delivery vehicle to topically deposit the cells onto the inner lumen of the de-epithelized rat trachea. Please click here to view a larger version of this figure.
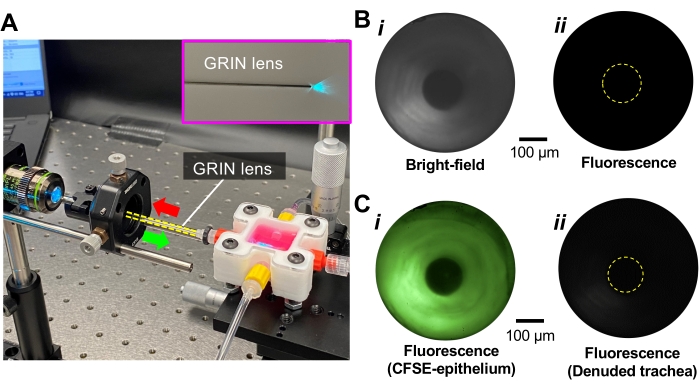
Figure 5: In situ imaging of de-epithelialized trachea. (A) Photograph showing fluorescent imaging of the trachea lumen while the CFSE-labeled epithelium is excited with 488 nm blue laser through GRIN lens. (B) (i) Bright-field and (ii) fluorescence images of the trachea lumen before epithelium labeling. (C) Fluorescence images of the (i) native and (ii) de-epithelialized trachea (De-Epi trachea) while the epithelium is labeled with CFSE fluorescent dye. Please click here to view a larger version of this figure.
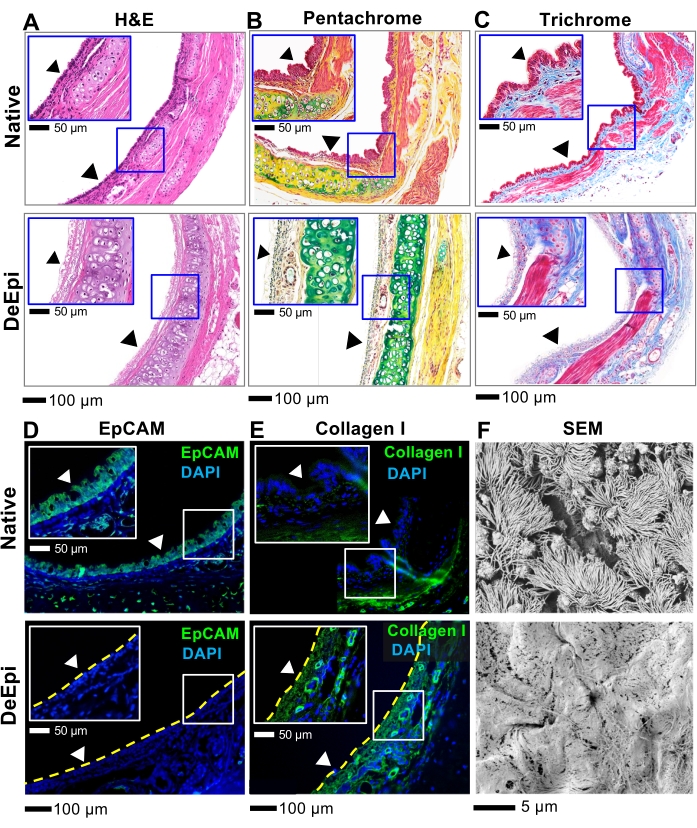
Figure 6: Histology, immunofluorescence, and SEM analyses of native and de-epithelialized rat tracheas. (A) H&E staining. (B) Pentachrome staining where purple is cell cytoplasm, blue is cell nuclei, green is proteoglycans (e.g., mucin), and yellow is collagen fibers. (C) Trichrome staining where pink is cell cytoplasm, dark blue is cell nuclei, and blue is collagen. Fluorescence images of native and de-epithelialized tracheas. (D) EpCAM and (E) collagen I. Arrowheads show the surface of the trachea lumen. (F) SEM micrographs of the trachea lumen. Please click here to view a larger version of this figure.
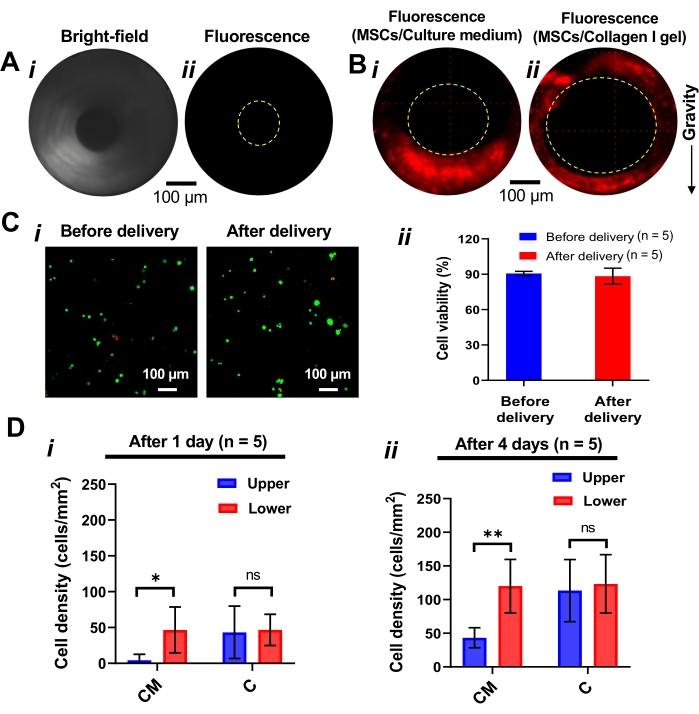
Figure 7: Topical deposition of the exogenous MSCs in the trachea lumen. (A) (i) Bright field and (ii) fluorescence images of the de-epithelialized trachea. (B) Fluorescent images of the de-epithelialized trachea lumen when it is seeded with (i) PBS and (ii) collagen I pre-gel. The homogenous distribution of the cells onto the trachea lumen is achieved when pre-gel collagen is used as a delivery vehicle for cells. (C) (i) Fluorescent images and (ii) quantified viability of the cells before and after 6 h of delivery by pre-gel collagen. n: number of samples. Steps 5.1 and 5.17 of the protocol were followed to assess the viability of the cells. (D) Cell seeding density measured after (i) 1 day and (ii) 4 days after cell seeding and culture. The cell density was calculated by dividing cell numbers by the examined surface area. All values represent mean ± standard deviation. One-way analysis of variance (ANOVA) was used to determine statistically significant differences between groups, with p < 0.05 considered significant. Abbreviations: CM = culture medium, C = collagen. *p < 0.05. **p < 0.01. ns: not significant. No significant difference (ns) between upper and lower surfaces means uniform cell distribution across the circumference of the trachea. Please click here to view a larger version of this figure.
