There were 67 patients enrolled in the study. As shown in Table 1, the mean age of the patients was 28.8 ± 3.7 years (range: 23-45 years). The time since herniorrhaphy was 24.5 ± 3.2 years (range: 21-43 years). The female partners were 25.2 ± 3.2 years (range: 23-42 years) years old. A total of 11 (16.4%) patients had pain in the scrotum. Four patients (6.0%) were underweight (BMI < 18.5 kg/m2), 53 (79.1%) had normal weight (BMI 18.5-24.9 kg/m2), eight (11.9%) were overweight (BMI 25-29.9 kg/m2), and two (3.0%) were obese (BMI > 30 kg/m2) .
In our study, the sites of obstruction were classified into three groups. (1) The obstruction of the vas deferens is at the incision of the original hernia repair (>2 cm); (2) the obstruction of the vas deferens is 2 cm higher than the original incision; (3) the obstruction of the vas deferens is more than 5 cm from the upper edge of the original incision. Table 2 shows the location of vas deferens obstruction and the results according to the surgical method in the different subgroups. The smear showed that 25 cases (37.3%) had no sperm in the cannula fluid. Of these, three (12.0%) underwent bilateral VV surgery with the obstruction site in the original incision, and the patency rate was 33.3% (one of three). In total, 22 (88.0%) underwent assisted reproductive technology (ART), in which the obstruction of the vas deferens was 2 cm higher than the upper edge of the original incision. The smear detected sperm in the fluid of the cannula needle in 42 (62.7%) cases. Of these, 29 (69.0%) underwent bilateral VV surgery with the obstruction site in the original incision, and the patency rate was 79.3% (23 of 29). A total of 10 (23.0%) underwent laparoscopy-assisted (lapa)-VV, with the obstruction site 2 cm higher than the original incision, and the patency rate was 40% (four of 10). A further three (7.10%) underwent seminal vesiculoscopy (SV), in which the obstruction site was 5 cm higher than the original incision, and the patency rates was 33.3% (one of three).
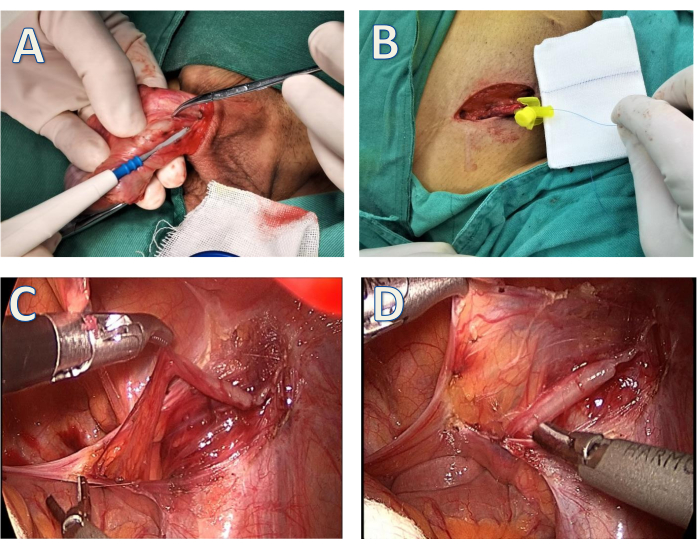
Figure 1: Schematic of the procedure. (A) The thickened vas deferens was separated. (B) A 3-0 polypropylene suture was passed through the cannula needle to probe the position of the obstructed site. (C) The vas deferens was identified beneath the peritoneum. (D) The vas deferens was mobilized with its blood supply off scar tissue. Please click here to view a larger version of this figure.
| Characteristics | N |
| Patient age, years | |
| Mean±SD | 28.8±3.7 |
| Range | 23-45 |
| Time since herniorrhaphy, years | |
| Mean±SD | 24.5±3.2 |
| Range | 21-43 |
| Female partner age, years | |
| Mean±SD | 25.2±3.2 |
| Range | 23-42 |
| With scrotal pain, n (%) | |
| Yes | 11(16.4%) |
| No | 56(83.6%) |
| BMI | |
| Underweight (<18.5 kg/m2) | 4(6.0%) |
| Normal (18.5-24.9 kg/m2) | 53(79.1%) |
| Overweight (25-29.9 kg/m2) | 8(11.9%) |
| Obese (≥30 kg/m2) | 2(3.0%) |
| BMI, body mass index. |
Table 1: Basic information of the patients. Abbreviation: BMI = body mass index. Data for this table is reprinted with permission from Wang et al.5
| Sperm exist in the vas deferens | Patients, n (%) | The site of obstruction | Patients, n (%) | Treatment (%) | Patency n (%) |
| No | 25(37.3) | < 2cm | 3(12.0) | MVE+MVV | 1(33.3) |
| >2cm | 22(88.0) | ART | – | ||
| Yes | 42(62.7) | <2cm | 29(69.0) | Bi-VV | 23(79.3) |
| >2cm | 10(23.8) | Lapa-VV | 4(40.0) | ||
| >5cm | 3(7.1) | SV | 1(33.3) |
Table 2: The site of vas deferens obstruction and the results based on operative manners in different subgroups. Abbreviations: MVE = microsurgical vasoepididymostomy; MVV = microsurgical vasovasostomy; Bi-VV = bilateral vasovasostomy; lapa-VV = laparoscopy-assisted vasovasostomy; SV = seminal vesiculoscopy; ART = assisted reproductive technology.
