The electrophysiological technique was performed on 48 patients from August to December 2021. Among them, 46 cases had penile temperature disorder with a temperature of 30.2 ± 1.2 °C, 35 cases had groin temperature disorder with a temperature of 30.6 ± 1.3 °C, and 18 cases had abdominal temperature disorder with a temperature of 30.1 ± 1.2 °C. After one course of treatment, the temperature of the treatment site increased in all patients. The temperature of the penis was 31.0 ± 1.0 °C, the temperature of the groin was 31.5 ± 1.1 °C, and the temperature of the lower abdomen was 31.2 ± 1.1 °C. The IIEF-5 score before treatment was 13.8 ± 3.6, and the IIEF-5 score after one course of treatment was 16.6 ± 4.2. The temperature and IIEF-5 score of the patient's treatment site were both increased after treatment (p < 0.05); the Erectile Hardness Scale (EHS) score, which showed a skewed distribution, was 2.43 (2, 3) versus 2.96 (2, 3.75). These differences were significant (p < 0.05) (Table 1).
The effect of this electrophysiological technique was analyzed via Audiovisual Sexual Stimulation (AVSS) examinations before and after therapy, as shown in Table 2. Before and after therapy, the erection time of the patients significantly increased from 6.14 (0.44, 11.5) min to 8.67 (4.13, 14.25) min (p < 0.01). The average hardness of the tip of the penis significantly increased from 18.92% (1.50%, 30.00%) to 24.33% (15.00%, 34.00%) (p < 0.01), as did the average hardness of the root of the penis, from 26.33% (5.75%, 39.50%) to 30.10% (26.00%, 41.50%) (p < 0.01). The circumference of the tip of the penis significantly increased from 1.30 (0, 2.15) cm to 1.67 (1.20, 2.20) cm (p < 0.05), whereas the circumference of the penis root increased from 1.70 (0.23, 2.58) cm to 1.79 (1.40, 2.6) cm (p > 0.05).
In an example, a 32-year-old male came to the hospital for medical treatment after experiencing weak erection and unsatisfactory sexual experience for 1 month. The patient met the inclusion criteria and volunteered to participate in this trial. Before the treatment, the IIEF-5 score of the patient was 17, and the erectile hardness monitor indicated poor hardness. The patient entered the medical infrared camera inspection chamber, followed the instructions as shown in Figure 1, and the infrared thermal imager analyzed the temperature of the patient's penis, groin, and lower abdomen with different movements. The infrared thermal imager indicated that the penis temperature was 32.7 °C, the groin temperature was 33.7 °C, and the lower abdomen temperature was 32.5 °C.
According to the examination, the patient's penis and lower abdomen were identified as the anomalous sites. Therefore, we affixed the electrodes to the corresponding sites on the patient and connected them to the computer equipment of the low-frequency neuromuscular therapy instrument as shown in Figure 3 and Figure 5. We observed the temperature change of each program acting on the abnormal points under infrared thermal imaging for 60 s, selected the fastest program for the temperature of the abnormal site to return to normal, and determined the corresponding frequency and pulse width on the low-frequency neuromuscular therapy instrument. The treatment plan for the patient was "30 Hz, 500 US" to stimulate the patient's penis and lower abdomen for 30 min in turn once a day, for a total of 12 stimulations as a course. After a course of treatment, the patient had satisfactory intercourse, with an IIEF-5 score of 21 and erectile hardness monitor indicating suitable hardness. The infrared thermal imager showed a penis temperature of 34.3 °C and a lower abdomen temperature of 33.1 °C.
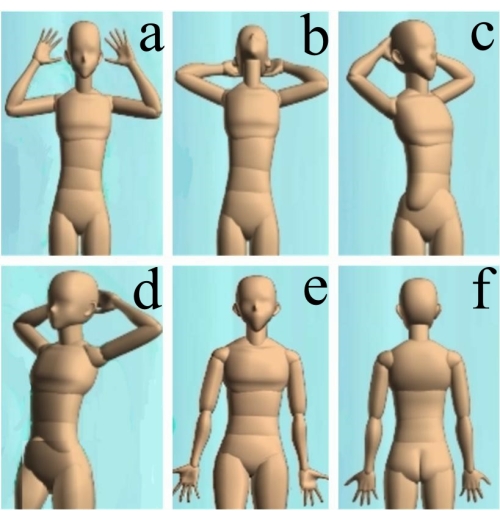
Figure 1: Actions to be followed by the patients. (A) Put the hands up against the ears and put the palms forward with fingers open. (B) Place the hands on the back of the head and lean back to reveal the neck. (C) Put the hands on the back of the head and turn 45° to the left. (D) Place the hands on the back of the head and turn 45° to the right. (E) Spread the legs slightly with drooping hands and put the palms forward with fingers open, facing the scanning head. (F) Keeping the hands down, put the palms forward with fingers open and face away from the scanning head. Please click here to view a larger version of this figure.
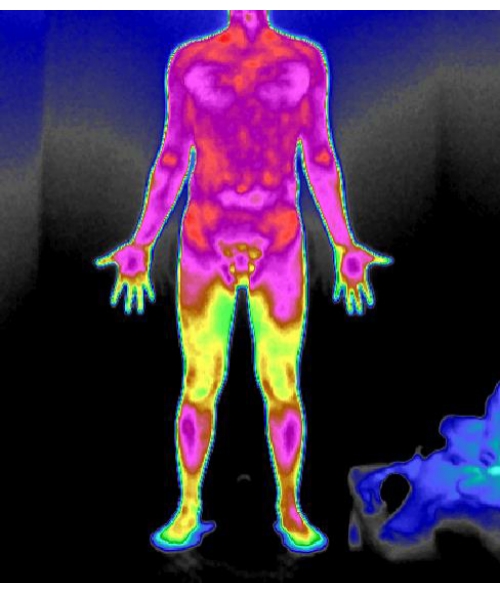
Figure 2: Normal infrared thermal imaging. Please click here to view a larger version of this figure.

Figure 3: Placement of electrode pads for abnormal penile temperature. Please click here to view a larger version of this figure.

Figure 4: Placement of electrode pads for abnormal groin temperature. Please click here to view a larger version of this figure.

Figure 5: Placement of electrode pads for abnormal abdominal temperature. Please click here to view a larger version of this figure.
| before therapy | after treatment | N | P | |
| temperature of penis (°C) | 30.2 ± 1.2 | 31.0 ± 1.0 | 46 | <0.05 |
| temperature of groin (°C) | 30.6 ± 1.3 | 31.5 ± 1.1 | 35 | <0.05 |
| temperature of lower abdomen (°C) | 30.1 ± 1.2 | 31.2 ± 1.1 | 18 | <0.05 |
| IIEF-5 | 13.8 ± 3.6 | 16.6 ± 4.2 | 48 | <0.05 |
| EHS | 2.43 (2, 3) | 2.96 (2, 3.75) | 48 | 0.02 |
Table 1: The effect of the electrophysiological technique on the temperature, IIEF-5, and EHS of the treatment site. Abbreviations: IIEF-5 = International Erectile Function Questionnaire-5; EHS = Erectile Hardness Scale.
| before therapy | after treatment | N | P | |
| erection time (min) | 6.14 (0.44, 11.5) | 8.67 (4.13, 14.25) | 48 | <0.05 |
| the average hardness of the tip (%) | 18.92 (1.50, 30.00) | 24.33 (15.00, 34.00) | 48 | 0.001 |
| the average hardness of the root (%) | 26.33 (5.75, 39.50) | 30.10 (26.00, 41.50) | 48 | <0.05 |
| the circumference of tip (cm) | 1.30 (0, 2.15) | 1.67 (1.20, 2.20) | 48 | 0.018 |
| the circumference of root (cm) | 1.70 (0.23, 2.58) | 1.79 (1.40, 2.6) | 48 | 0.272 |
Table 2: The effect of the electrophysiological technique on the results of the AVSS examination in ED patients. Abbreviations: AVSS = AudioVisual Sexual Stimulation; ED = erectile dysfunction.
