A Mouse Model of Orotracheal Intubation and Ventilated Lung Ischemia Reperfusion Surgery
Summary
A mouse surgical model to create left lung ischemia reperfusion (IR) injury while maintaining ventilation and avoiding hypoxia.
Abstract
Ischemia reperfusion (IR) injury frequently results from processes that involve a transient period of interrupted blood flow. In the lung, isolated IR permits the experimental study of this specific process with continued alveolar ventilation, thereby avoiding the compounding injurious processes of hypoxia and atelectasis. In the clinical context, lung ischemia reperfusion injury (also known as lung IRI or LIRI) is caused by numerous processes, including but not limited to pulmonary embolism, resuscitated hemorrhagic trauma, and lung transplantation. There are currently limited effective treatment options for LIRI. Here, we present a reversible surgical model of lung IR involving first orotracheal intubation followed by unilateral left lung ischemia and reperfusion with preserved alveolar ventilation or gas exchange. Mice undergo a left thoracotomy, through which the left pulmonary artery is exposed, visualized, isolated, and compressed using a reversible slipknot. The surgical incision is then closed during the ischemic period, and the animal is awakened and extubated. With the mouse spontaneously breathing, reperfusion is established by releasing the slipknot around the pulmonary artery. This clinically relevant survival model permits the evaluation of lung IR injury, the resolution phase, downstream effects on lung function, as well as two-hit models involving experimental pneumonia. While technically challenging, this model can be mastered over the course of a few weeks to months with an eventual survival or success rate of 80%-90%.
Introduction
Ischemia reperfusion (IR) injury can occur when blood flow is restored to an organ or tissue bed after some period of interruption. In the lung, IR can occur in isolation or in association with other injurious processes such as infection, hypoxia, atelectasis, volutrauma (from high tidal volumes during mechanical ventilation), barotrauma (high peak or sustained pressures during mechanical ventilation), or blunt (non-penetrating) lung contusion injury1,2,3. There remain several gaps in our knowledge about the mechanisms of LIRI and the impact of concurrent processes (e.g., infection) on LIRI outcomes, and also the treatment options for LIRI are limited. An in vivo model of pure LIRI is required to identify the pathophysiology of lung IR injury in isolation and to study its contribution to any multi-hit process of which lung injury is a component.
Murine lung IR models can be used to study the lung-specific pathophysiology of multiple processes, including lung transplantation3, pulmonary embolism4, and lung injury following hemorrhagic trauma with resuscitation5. Currently used models include surgical lung transplantation6, hilar clamping7, ex vivo lung perfusion8, and ventilated lung IR9. Here, we provide a detailed protocol for a murine ventilated lung IR model of sterile lung injury. There are multiple benefits of this approach (Figure 2), including that it induces minimal hypoxia and minimal atelectasis, and it is a survival surgery model that allows for long-term studies.
Reasons to choose this model of LIRI over other models such as the hilar clamping and ex vivo perfusion models are the following: this model minimizes the inflammatory contributions of atelectasis, mechanical ventilation, and hypoxia; it preserves cyclical ventilation; it maintains an intact in vivo circulatory immune system that can respond to the IR injury; and finally, as a survival procedure, it permits the longer-term analysis of the mechanisms of secondary injury generation (2-hit models) and injury resolution. Overall, we believe this ventilated lung IR model provides the "purest" form of IR injury that can be studied experimentally.
Other publications have described the use of orotracheal intubation of mice to perform IT injections or installations10,11, but not as the starting point for a survival surgery as it is in this model. The placement of an orotracheal tube permits the performance of lung surgery by allowing the collapse of the operative lung. It also allows for the reinflation of the lung at the end of the procedure, which is critical for the pneumothorax and for the ability of the mouse to return to spontaneous ventilation at the conclusion of the procedures. Finally, the removal of the secured orotracheal tube is a simple procedure that, unlike an invasive tracheotomy, is compatible with a survival surgery. This allows for longer term research studies focused on understanding the progression and resolution of LIRI and associated disorders, as well as the creation of chronic injury models.
Protocol
All procedures and steps described below were approved by the institutional animal care and use committee (IACUC) at the University of California San Francisco. Any mouse strain can be used, though some strains have a more robust lung IR inflammatory response compared to others12. Mice that are approximately 12-15 weeks of age (30-40 g) or older tolerate and survive the lung IR surgery better than younger mice. Both male and female mice can be used for these surgeries.
1. Mouse Intubation Protocol
- Anesthesia and preparation for intubation
- Wipe the mouse abdomen with an ethanol swab. Anesthetize the mouse with an intraperitoneal injection of tribromoethanol (250-400 mg/kg). Assess the appropriate depth of anesthesia by the lack of pedal withdrawal reflex. Place eye lubricating ointment now or later (step 2.1.4).
NOTE: For this procedure, tribromoethanol (and etomidate as an alternative option) provides a stable anesthetic plane without affecting the hemodynamic conditions required for this surgery. This anesthetic is only used once to avoid the risk of peritoneal adhesions. Isoflurane could also be used, but we do not use it here. The practitioner is free to use whatever anesthetic recipe they see fit. - Place the anesthetized mouse on an intubation stand or plastic support in a supine position, suspended by its upper incisors on looped 4-0 sutures (silk or other) across two support anchors.
- To keep the mouse immobilized during the intubation procedure, loosely tape the lower part of the chest (or both upper limbs) to the platform.
- Place the fiberoptic flexible light gently on the trachea of the mouse, slightly below the vocal cords. Adjust the level of illumination so that only a dark field is visible when looking into the mouse oropharynx except for red light emanating from below the vocal cords, demonstrating the target for the eventual placement of the endotracheal tube. Note that vocal cord movements should be visible with the naked eye or, if needed, under magnification.
- Wipe the mouse abdomen with an ethanol swab. Anesthetize the mouse with an intraperitoneal injection of tribromoethanol (250-400 mg/kg). Assess the appropriate depth of anesthesia by the lack of pedal withdrawal reflex. Place eye lubricating ointment now or later (step 2.1.4).
- Intubation procedure
- Hold the tweezers with the dominant hand and use them to gently grip and draw the tongue out of the oral cavity.
- Open the lower jaw using forceps held by the non-dominant hand, and then push the forceps into the larynx to gently lift the epiglottis. At this time, release the tongue from the tweezers.
- Look for the vocal cords. They should open and close according to each breath. Holding the cannula with the guide wire pre-loaded, insert the tip of the wire through the vocal cords.
- Being very careful not to move the wire by holding a portion of it that is outside the cannula but just above the vocal cords, withdraw the cannula, leaving just the wire in place with its distal end within the trachea.
- At this point, perform a second visualization of the vocal cords to confirm that the wire distal tip remains passed through the illuminated vocal cords and into the trachea, and is not in the unlit esophagus.
- Hold the wire outside the mouth with the curved forceps in the left hand, stabilized against a hard surface, and carefully advance the 20G catheter with tape wings over the wire.
- Once the distal end of the wire emerges from the back end of the 20G catheter or endotracheal tube, hold that end with the curved forceps and smoothly advance the 20G catheter into the trachea.
- Carefully remove the wire from the distal end of the 20G catheter with the curved forceps without dislodging the placement of the catheter.
- Briefly connect the catheter to the ventilator before securing it to confirm proper placement into the trachea and not the esophagus. Confirm tracheal placement by observation of mechanical ventilation-dependent bilateral chest wall movements and the absence of inflation of the stomach.
- Post-intubation
- Disconnect the catheter from the ventilator. Fix the tape wings (attached to the catheter) through the lower lip of the mouse using a 4-0 vicryl suture to firmly secure the endotracheal tube (ETT) to the mouse during all subsequent procedures/manipulations.
NOTE: Alternatively, silk tape or other tape can be used to secure the ETT, however care should be taken to avoid dislodgement of the ETT during movement of the animal from the intubation sled to the surgical surface. - Carefully remove the mouse from the intubation sled. Briefly connect the catheter to the ventilator set at a tidal volume 0.2-0.225 mL and a respiratory rate of 120-150 breaths per min to confirm correct tracheal placement of the orotracheal tube and then disconnect with the mouse breathing spontaneously through the orotracheal tube.
- Do not leave the animal unattended from this point onward until it has regained sufficient consciousness to maintain sternal recumbency at the end of the procedure.
- Disconnect the catheter from the ventilator. Fix the tape wings (attached to the catheter) through the lower lip of the mouse using a 4-0 vicryl suture to firmly secure the endotracheal tube (ETT) to the mouse during all subsequent procedures/manipulations.
2. Lung ischemia and reperfusion (IR) surgery protocol
- Analgesia and preparation of the surgical site
- Wipe the mouse abdomen with an ethanol swab and inject buprenorphine (0.05-0.1 mg/kg) intraperitoneally.
- Shave the hair over the left thorax area up to the left scapula. Remove excess shaved hair using alcohol swabs.
NOTE: Steps 2.1.1 and 2.1.2 can also be performed before intubation if there concern for dislodgement of the ETT when secured with silk tape. - Place the mouse on a warming pad in a left lateral or 3/4 turned position and connect the tracheal tube on the ventilator with a tidal volume of 0.2-0.225 mL (~8 mg/kg) and a respiratory rate of 120-150 breaths per min. Do not use supplemental oxygen for this procedure.
- Apply eye lubricant with a sterile cotton-tip swab. Turn the mouse to 3/4 left side up and immobilize all four limbs and the tail with laboratory tape.
- Disinfect the shaved skin area and surrounding fur with povidone-iodine and wait for the solution to dry. Then cover the surgical field with a sterile drape or clear plastic film and create a rectangular opening in the drape or plastic film for the surgical field.
- Surgical procedure
- Confirm the appropriate level of anesthesia (provided by the administration of tribromoethanol and buprenorphine as described earlier) by testing response to toe pinch.
- Using a pair of sharp scissors and a pair of larger forceps (narrow pattern forceps or similar), make a 2 cm transverse skin incision below the inferior angle of the scapula in the left lateral thorax. Use the scissors and a finer pair of forceps (extra fine graefe forceps or similar) to cut into the muscular layer and dissect down to the ribs.
- Identify the second intercostal space and hold the second rib with the extra fine forceps. Pulling the rib upward, use a sterile #11 or #12 (curved) scalpel blade (no handle necessary) to enter the pleural space by separating and cutting across the 2nd-3rd space's intercostal muscles. Consider pausing ventilation to reduce injury to the left lung apex.
- Insert three sterilized retractors. Use the smallest/narrowest retractor cephalad along the orientation of the ribs, the medium size retractor to the left along the 2nd rib, and the largest retractor to the right along the surface of the 3rd rib.
- Open the chest with slow and progressive retraction using the elastic retractor cords. Expose and identify the left pulmonary artery (PA) by moving the left lung apex away with a sterile cotton-tip swab.
- Use the micro forceps, ultrafine forceps in the right hand and PA or vessel dilating forceps in the left hand, to gently expose and create the field in which the left PA and bronchus are both visible.
- Using the PA forceps, pick up the left PA and pull gently but firmly upward and cephalad to visualize the transparent bronchus below. Increase magnification on the dissection microscope (see equipment list for more details) at this point to maximum (2x).
NOTE: Sterilize all equipment before use. Additionally, to maintain sterility, only the tips of surgical instruments should enter the sterile surgical field. - While retracting the PA away from the bronchus, carefully pass the closed ultrafine forceps through the space between the left PA and bronchus. Then, use these forceps to hold and pull a 7-0 or 8-0 prolene suture through the space between the left pulmonary artery (above) and bronchus (below).
- Encircle the left PA by tying a slipknot to create an occlusion in the PA. Blood flow interruption is easily visualized under the microscope. This marks the initiation of the ischemic period.
- Externalize the free end of the knot through a different entry point in the anterior left thorax using a 24G-28G needle and secure the end of the suture with a small piece of tape for easier identification later on.
- Reinflate the lung to expel as much air out of the chest cavity as possible using a PEEP valve/tubing on the rodent ventilator. Then, close the ribcage with two interrupted 4-0 nylon sutures.
- Close the muscle and subcutaneous layer with a running 4-0 nylon suture. Then apply two or three drops of topical bupivacaine (0.5%) to the incision. Use a 4-0 nylon suture to close the skin layer with a running suture.
- Post-operative care
- When spontaneous ventilation has resumed, disconnect the endotracheal tube from the ventilator and extubate the mouse.
- Place the mouse on the warming pad to maintain body temperature during early post-anesthesia recovery.
- Carefully monitor the mouse while recovering from general anesthesia. Pull the externalized slipknot gently at the end of the ischemic period (30 min or 1 h).
- Move the mouse from the warming pad to a cage once it has exhibited signs of recovery: self-righting and/or movement.
- After the period of reperfusion (1 h or 3 h), euthanize the animal and collect blood by cardiac puncture and lung tissue for further analysis. For 1 h reperfusion, collect plasma for ELISA, tissue for RNA, and protein analysis; for 3 h reperfusion, additionally collect tissue for histology.
Representative Results
Inflammation generated by unilateral ventilated sterile lung ischemia reperfusion (IR) injury: Following 1 h of ischemia, we observed increased levels of cytokines in the serum and within the lung tissue by both ELISA and qRT-PCR that peaked at 1 h following reperfusion and rapidly returned to baseline within 12-24 h after reperfusion13. For samples collected at 3 h following reperfusion, we observed intense neutrophil infiltration within the left lung tissue and noted that the intensity of the inflammation was dependent on the strain of mouse used (Figure 1). Notably, the inflammation that is generated in the absence of a co-existing or subsequent infectious process gradually resolves and the lungs return to their normal lung architecture (by histopathology) with efferocytosis or egress of neutrophils from the injured lungs within 12-24 h after reperfusion13. Of note, we observed mild but detectable inflammation, which was largely neutrophilic and was observed in the non-operative right lung as well, which we hypothesize is due to hyperperfusion injury14.
Tissue sample collection for this lung IR model is no different than that for other lung IR models: blood can be collected for plasma preparation via cardiac puncture or IVC cannulation; lung tissue can be harvested for protein or RNA preparation and then for further analysis by western blot, ELISA, or qPCR.
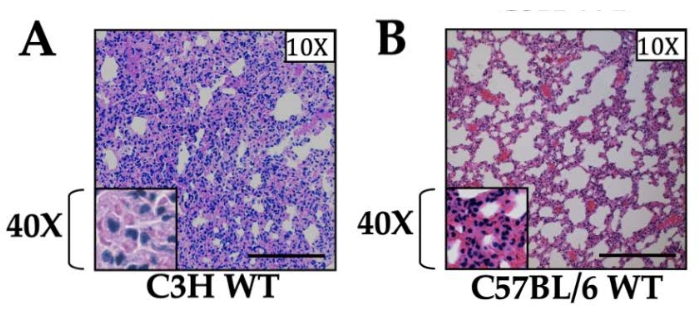
Figure 1: Histology of lung sections in wild type mice of two different strains. (A) C3H and (B) C57BL/6 mice. Both strains of mice received 1 h ischemia and 3 h reperfusion, and the tissue is shown at 10x magnification. The 40x magnification is shown in the inset. Neutrophilic infiltration was observed in both strains, with the C3H strain showing markedly greater levels of inflammation compared to C57BL/6 as reported earlier12. Scale bar is 200 µm. Please click here to view a larger version of this figure.
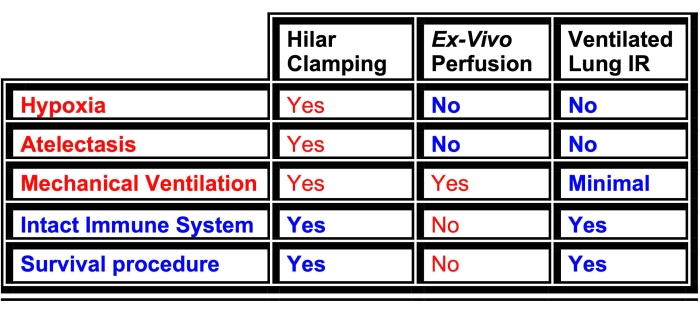
Figure 2: Comparison of advantages (blue text) and disadvantages (red text) of the three most commonly used mouse experimental lung IR injury (LIRI) models. This comparison highlights the choice of ventilated lung IR (described in this manuscript) as the ideal model for studying pure lung IR. Please click here to view a larger version of this figure.
Discussion
This manuscript details the steps involved in performing the ventilated lung IR model developed by Dodd-o et al.9. This model has helped identify molecular pathways involved in the generation and resolution of inflammation from lung IR in isolation14,15,16,17, lung IR in combination with co-existing infection18, and lung IR in relation to the gut-lung axis and the contribution of the gut microbiome13,18,19. While technically more challenging, the current model allows for the evaluation of lung IR without the compounding effects of interrupted cyclic lung inflation and hypoxia. It also minimizes the period of mechanical ventilatory exposure, unlike the ex vivo perfusion model, which itself can lead to lung injury20.
Limitations of the method: While the mouse trachea is tapered enough that positive end expiratory pressure (PEEP) allows for expansion of the lungs and provides a snug fit for the ETT, lung mechanics and flow-volume loop measurements may not be possible with this version of reversible orotracheal intubation. These lung physiology measurements may require a tracheotomy, which, unlike this method, is incompatible with a survival lung surgery. Reversible orotracheal intubation is well tolerated by mice, and even in the absence of paralytics there is very little mouse-ventilator asynchrony provided the minute ventilation (MV = tidal volume x respiratory rate) is sufficiently high enough to prevent the natural CO2-driven drive by the breath taking over (i.e., just beyond the apneic threshold).
There are several considerations related to the ischemia-reperfusion (IR) portion of this procedure. First, the IR procedure should be performed with as little physical trauma to the lung as possible. We recommend pausing the mechanical ventilation and allowing the mouse to breathe spontaneously when entering the thoracic cavity. The negative pressure ventilation, along with the surgeon's grasping of the second or third rib and pulling it away from the lung while carefully entering the chest with a #11 scalpel blade, will reduce the chance of injuring the lung with the scalpel. Alternatively, we have found that using a #12 curved scalpel blade, positioned so that the curve faces upward, allows for more careful entry into the thoracic cavity, potentially reducing injury to the underlying left lung apex surface. Additionally, the connection between the left PA and the bronchus is less secure closer to the hilum, making passage of the ultrafine forceps between these two structures easier here.
The next critical step is isolating the left PA from the bronchus below to encircle the PA with a suture tie. It is essential that this step be accomplished carefully to avoid trauma to the lung apex. We recommend entering the thoracic cage as cephalad as possible to minimize the amount of the left lung that needs to be displaced or retracted to access the PA and bronchus. Any part of the lung that sustains blunt trauma must be excluded from evaluation for isolated IR injury. Often, the apex of the left lung is excised away when collecting the lungs for final analysis of sterile lung IR injury. Injury of the apex of the lung can be visualized during the surgery due to the presence of puncta of hemorrhage or bloody discoloration.
Between the PA and the bronchus below exists a connective tissue layer that must be breached to encircle the artery with the suture tie. Learning how much tension is permitted while grasping and pulling the left PA upward (i.e., toward the thoracic cage and away from the bronchus), using the non-serrated, non-damaging vessel grasping flat fine forceps in the left hand, is an important first step to master. The left PA can tolerate a surprising amount of tension and stretch as it is pulled upward. We find it helpful to increase magnification of the visual field to maximum and adjusting focus so that the potential space (a white line of connective tissue adhering the PA to the bronchus) can be clearly and sharply visualized along with the ultrafine forceps (held in the right hand). For the field to remain in focus, it is important to stabilize the left hand on the surgical surface while pulling the left PA up and away from the bronchus. The ultrafine forceps can then be passed in the space between the two structures. The closed tips should pass easily without any real resistance, and once seen on the other side of the left PA, the tips can be opened gently to further create space for the passage of the suture material. It is critical that this be performed using completely undamaged ultrafine forceps, which can be quickly determined by pulling a sterile alcohol swab through the closed tips to observe whether the tips tear at the material. Damage tips can also be identified by opening and closing the forceps under maximal magnification of the surgical microscope.
It is easy to detect damage that occurs to either the left PA or left main bronchus while attempting to separate them. Damage to the left PA results in flooding of the visual field with blood and can result in a non-salvageable surgery if the damage creates a hole within the PA itself. Notably, there are surface microscopic blood vessels on the PA that may get injured during the ultrafine forceps movement and can potentially be managed by placing a dry sterile cotton-tip swab over the field to absorb the blood that appears. If the bleeding stops, the procedure can be resumed. Damage to the left main bronchus is always a non-salvageable situation since there is no simple or rapid way of repairing airway damage.
The step of separating the PA from the underlying bronchus can be initially practiced on a dead mouse without the pressure of time or the distraction of cardiac activity and the movement it causes. Additionally, the stasis of blood in the left PA allows for it to be more easily visualized (thick and plump vessel), and yet still capable of being picked up by the non-injuring flat PA forceps. The ability to detect damage in the left bronchus is still possible, since the ventilation of the left lung can be used to assess for the presence of an intact conducting airway to the left lung. This practice situation can also be used to perfect the creation of the slipknot.
There is a finite duration of occlusion, beyond which spontaneous reperfusion after removal of the slipknot is not guaranteed. In pilot studies, this occurs somewhere between 6 and 10 h. Beyond this, reperfusion occurs less immediately after removal of the slipknot. As the ischemic period extends, reperfusion requires manipulation of the PA after slipknot removal in order to re-establish blood flow.
These following observations have been obtained from five co-authors of this paper that represent their collective experience in learning, perfecting, troubleshooting, and improving this procedure during the period when they conducted this mouse surgical model and have been summarized in the points below:
On average, it took 1-3 months to master this surgical procedure. One proceduralist estimated that it takes approximately 50 surgeries to become facile with the different procedures.
Success rate at the start of performing the procedure was 20%-40%. After performing the procedure regularly and with familiarity, success rate increased to 80%-90%.
The most difficult part of the surgery was unanimously the passing of the ultrafine forceps between the left PA and the left bronchus, and then the subsequent capture of the suture monofilament with the forceps and its passing between the two structures.
Mistakes during the passage of the monofilament between the PA and left mainstem bronchus can lead to an unsalvageable surgery with catastrophic bleeding of the left PA or irreversible injury to the left main bronchus.
The maximum number of surgeries feasible in 1 single day was estimated to be 10 (at approximately 35-45 min/surgery), while the ideal number for proceduralist comfort and surgical success was five or six.
Other miscellaneous tips and suggestions include:
Avoid excess caffeine before starting the surgical day to maintain steady hand position.
Increase magnification on the microscope to maximum during the portion of the procedure when the suture is being passed between the left PA and left main bronchus.
Use gentle and gradual/incremental movements when advancing the Dumont forceps to create space between the left PA and left main bronchus.
Stabilize hands on the surgical surface when performing all critical steps.
Ensure that the respiratory rate on the ventilator is high enough to avoid spontaneous breaths, especially during the key/critical portions of the procedure (suture passing between the left PA and left main bronchus).
A quiet and undisturbed environment to perform the surgeries is essential to stay focused and undistracted.
Figure 2 compares this model to alternative models of lung IR injury. This model of ventilated lung ischemia reperfusion offers the advantages of minimizing atelectasis, hypoxia, and mechanical ventilation. Importantly, as a survival surgery, it is compatible with second injury models (e.g., experimental pneumonia models) and analysis of the resolution of injury.
In conclusion, we have described a survival surgery involving the creation of lung ischemia reperfusion injury that we believe can provide valuable insight into the mechanisms and cellular pathways involved in pure IR injury in the lung.
Divulgazioni
The authors have nothing to disclose.
Acknowledgements
This work was funded by departmental support from the Department of Anesthesia and Perioperative Care, University of California San Francisco and San Francisco General Hospital, as well as by an NIH R01 award (to AP): 1R01HL146753.
Materials
| Equipment | |||
| Fiber Optic Light Pipe | Cole-Parmer | UX-41720-65 | Fiberoptic light pipe |
| Fiber Optic Light Source | AmScope | SKU: CL-HL250-B | Light source for fiberoptic lights |
| Germinator 500 | Cell Point Scientific, Inc. | No.5-1450 | Bead Sterilizer |
| Heating Pad | AIMS | 14-370-223 | Alternative option |
| Lithium.Ion Grooming Kits(hair clipper) | WAHL home products | SKU 09854-600B | To remove mouse hair on surgical site |
| Microscope | Nikon | SMZ-10 | Other newer options available at the company website |
| MiniVent Ventilator | Havard Apparatus | Model 845 | Mouse ventilator |
| Ultrasonic Cleaner | Cole-Parmer | UX-08895-05 | Clean tools that been used in operation |
| Warming Pad | Kent Scientific | RT-0501 | To keep mouse warm while recovering from surgery |
| Weighing Scale | Cole-Parmer | UX-11003-41 | Weighing scale |
| Surgery Tools | |||
| 4-0 Silk Suture | Ethicon | 683G | For closing muscle layer |
| 7-0 Prolene Suture | Ethicon Industry | EP8734H | Using for making a slip knot of left pulmonary artery |
| Bard-Parker (11) Scalpel (Rib-Back Carbon Steel Surgical Blade, sterile, single use) | Aspen Surgical | 372611 | For entering thoracic cavity (option 1) |
| Bard-Parker (12) Scalpel | Aspen Surgical | 372612 | For entering thoracic cavity (option 2) |
| Extra Fine Graefe Forceps | FST | 11150-10 | Muscle/rib holding forceps |
| Magnetic Fixator Retraction System | FST | 1. Base Plate (Nos. 18200-03) 2. Fixators (Nos. 18200-01) 3. Retractors (Nos. 18200-05 through 18200-12) 4. Elastomer (Nos.18200-07) 5. Retractor(No.18200-08) |
Small Animal Retraction System |
| Monoject Standard Hypodermic Needle | COVIDIEN | 05-561-20 | For medication delivery IP |
| Narrow Pattern Forceps | FST | 11002-12 | Skin level forceps |
| Needle holder/Needle driver | FST | 12565-14 | for holding needles |
| Needles | BD | 305110 | 26 gauge needle for externalizing slipknot (24 or 26 gauge needle okay too) |
| PA/Vessel Dilating forceps | FST | 00125-11 | To hold PA; non-damaging gripper |
| Scissors | FST | 14060-09 | Used for incision and cutting into the muscular layer durging surgery |
| Ultra Fine Dumont micro forceps | FST | 11295-10 (Dumont #5 forceps, Biology tip, tip dimension:0.05*0.02mm,11cm) | For passing through the space between the left pulmonary artery and bronchus |
| Reagents | |||
| 0.25% Bupivacaine | Hospira, Inc. | 0409-1159-02 | Topical analgesic used during surgical wound closure |
| Avertin (2,2,2-Tribromoethanol) | Sigma-Aldrich | T48402-25G | Anesthetic, using for anesthetize the mouse for IR surgery, the concentration used in IR surgery is 250-400 mg/kg. |
| Buprenorphine | Covetrus North America | 59122 | Analgesic: concentration used for surgery is 0.05-0.1 mg/kg |
| Eye Lubricant | BAUSCH+LOMB | Soothe Lubricant Eye Ointment | Relieves dryness of the eye |
| Povidone-Iodine 10% Solution | MEDLINE INDUSTRIES INC | SKU MDS093944H (2 FL OZ, topical antiseptic) | Topical liquid applied for an effective first aid antiseptic at beginning of surgery |
| Materials | |||
| Alcohol Swab | BD brand | BD 326895 | for sterilzing area of injection and surgery |
| Plastic film | KIRKLAND | Stretch-Tite premium | Alternative for covering the sterilized surgical field (more cost effective) |
| Rodent Surgical Drapes | Stoelting | 50981 | Sterile field or drape for surgical field |
| Sterile Cotton Tipped Application | Pwi-Wnaps | 703033 | used for applying eye lubricant |
| Top Sponges | Dukal Corporaton | Reorder # 5360 | Stopping bleeding from skin/muscle |
Riferimenti
- Shen, H., Kreisel, D., Goldstein, D. R. Processes of sterile inflammation. Journal of Immunology. 191 (6), 2857-2863 (2013).
- Fiser, S. M., et al. Lung transplant reperfusion injury involves pulmonary macrophages and circulating leukocytes in a biphasic response. The Journal of Thoracic and Cardiovascular Surgery. 121 (6), 1069-1075 (2001).
- Lama, V. N., et al. Models of lung transplant research: A consensus statement from the National Heart, Lung, and Blood Institute workshop. JCI Insight. 2 (9), 93121 (2017).
- Miao, R., Liu, J., Wang, J. Overview of mouse pulmonary embolism models. Drug Discovery Today: Disease Models. 7 (3-4), 77-82 (2010).
- Mira, J. C., et al. Mouse injury model of polytrauma and shock. Methods in Molecular Biology. 1717, 1-15 (2018).
- Krupnick, A. S., et al. Orthotopic mouse lung transplantation as experimental methodology to study transplant and tumor biology. Nature Protocols. 4 (1), 86-93 (2009).
- Gielis, J. F., et al. A murine model of lung ischemia and reperfusion injury: Tricks of the trade. The Journal of Surgical Research. 194 (2), 659-666 (2015).
- Nelson, K., et al. Animal models of ex vivo lung perfusion as a platform for transplantation research. World Journal of Experimental Medicine. 4 (2), 7-15 (2014).
- Dodd-o, J. M., Hristopoulos, M. L., Faraday, N., Pearse, D. B. Effect of ischemia and reperfusion without airway occlusion on vascular barrier function in the in vivo mouse lung. Journal of Applied Physiology. 95 (5), 1971-1978 (2003).
- Lawrenz, M. B., Fodah, R. A., Gutierrez, M. G., Warawa, J. Intubation-mediated intratracheal (IMIT) instillation: a noninvasive, lung-specific delivery system. Journal of Visualized Experiments. (93), e52261 (2014).
- Rayamajhi, M., et al. Non-surgical intratracheal instillation of mice with analysis of lungs and lung draining lymph nodes by flow cytometry. Journal of Visualized Experiments. (51), e2702 (2011).
- Dodd-o, J. M., Hristopoulos, M. L., Welsh-Servinsky, L. E., Tankersley, C. G., Pearse, D. B. Strain-specific differences in sensitivity to ischemia-reperfusion lung injury in mice. Journal of Applied Physiology. 100 (5), 1590-1595 (2006).
- Prakash, A., et al. Lung ischemia reperfusion (IR) is a sterile inflammatory process influenced by commensal microbiota in mice. Shock. 44 (3), 272-279 (2015).
- Prakash, A., et al. Alveolar macrophages and toll-like receptor 4 mediate ventilated lung ischemia reperfusion injury in mice. Anesthesiology. 117 (4), 822-835 (2012).
- Dodd-o, J. M., et al. The role of natriuretic peptide receptor-A signaling in unilateral lung ischemia-reperfusion injury in the intact mouse. American Journal of Physiology. Lung Cellular and Molecular Physiology. 294 (4), 714-723 (2008).
- Prakash, A., Kianian, F., Tian, X., Maruyama, D. Ferroptosis mediates inflammation in lung ischemia-reperfusion (IR) sterile injury in mice. American Journal of Respiratory and Critical Care Medicine. 201, (2020).
- Tian, X., et al. NLRP3 inflammasome mediates dormant neutrophil recruitment following sterile lung injury and protects against subsequent bacterial pneumonia in mice. Frontiers in Immunology. 8, 1337 (2017).
- Tian, X., Hellman, J., Prakash, A. Elevated gut microbiome-derived propionate levels are associated with reduced sterile lung inflammation and bacterial immunity in mice. Frontiers in Microbiology. 10, 159 (2019).
- Liu, Q., Tian, X., Maruyama, D., Arjomandi, M., Prakash, A. Lung immune tone via gut-lung axis: Gut-derived LPS and short-chain fatty acids’ immunometabolic regulation of lung IL-1β, FFAR2, and FFAR3 expression. American Journal of Physiology. Lung Cellular and Molecular Physiology. 321 (1), 65-78 (2021).
- Dodd-o, J. M., et al. Interactive effects of mechanical ventilation and kidney health on lung function in an in vivo mouse model. American Journal of Physiology. Lung Cellular and Molecular Physiology. 296 (1), 3-11 (2009).
