After successful TAC surgery, pressure overload was detected using an ultrasound imaging system. Four weeks after surgery, mice develop decreased heart function. In the present study, the efficacy of TAC surgery was validated via ejection fraction (EF), fractional shortening (FS), left ventricular mass (LV mass) and left ventricular internal diameter (LVID) of mice who underwent TAC surgery after 4 weeks. EF was significantly reduced in TAC mice after 4 weeks compared to sham mice (47% ± 10% vs. 78% ± 4%, p < 0.0001) (Figure 4A). LV mass was significantly elevated in TAC mice (158.1 ± 50.5 vs. 91.8 ± 21.7 mg, p = 0.0226) (Figure 4B). FS was significantly reduced in TAC mice (23 ± 5 vs. 46% ± 3%, p < 0.0001) (Figure 4C). LVID was significantly elevated in TAC mice (2.88 ± 0.39 vs. 1.81 ± 0.52 mm, p = 0.0044) (Figure 4D). Data represents six mice each for TAC and Sham groups. Due to the small invasive procedures, the survival rate is rather high and mainly dependent on bleeding, which can be reduced to less than 5% for a skilled performer. When fully mastered, the general survival rate presented in C57BL/6J mice after 4 weeks is over 95%. An unpaired t-test was performed to compare the sham and TAC groups. All data are presented as mean ± SEM (error bars).
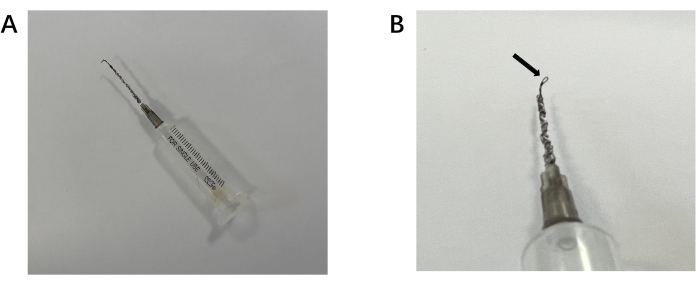
Figure 1: Self-made snare containing retractor for passing silk suture around the aortic arch. (A) Overall view of the retractor.(B) Detail of the retractor. Arrow indicates the snare for the silk to pass through. Please click here to view a larger version of this figure.
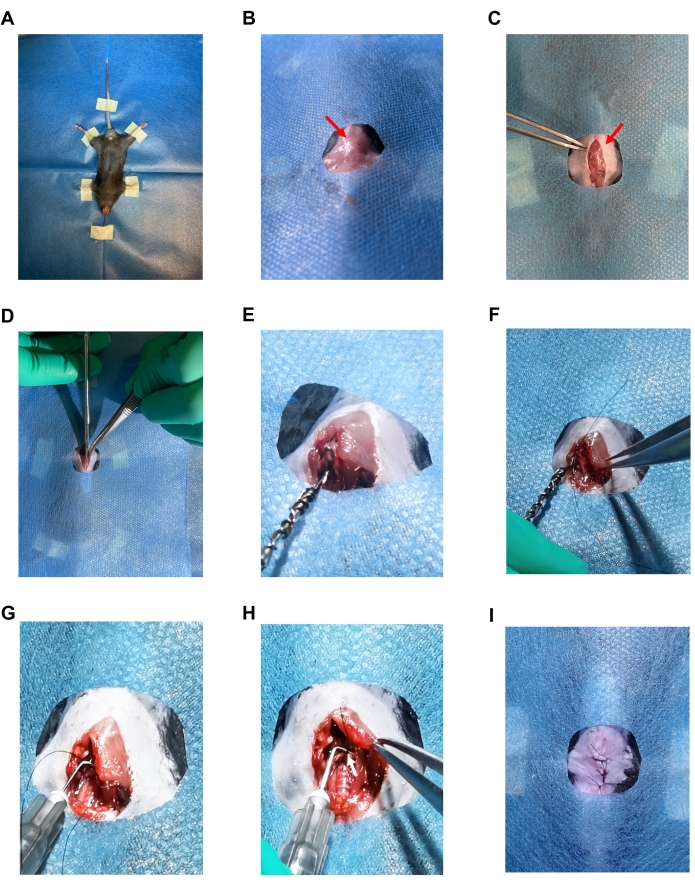
Figure 2: Images of the TAC surgery. (A) Supine position mouse fixed with tape and suture. (B) Sterile drape showing only the surgical area. (C) 1.5 cm vertical skin incision. The red arrow indicates a sternal angel. (D) Longitudinal midline incision that was made to the sternum. (E) Image showing the snare of the self-made retractor passing under the aorta. (F) Image showing the 7-0 silk suture passing through the snare loop. (G) A 27 G needle that was placed parallel to the aorta. (H) Ligation of the aorta with the 27 G needle. The white arrow indicates a ligation knot. (I) Sutured skin with 4-0 silk suture. Please click here to view a larger version of this figure.
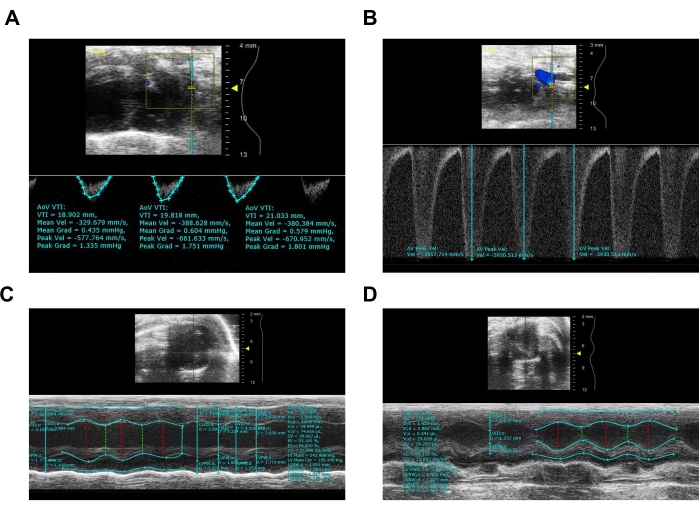
Figure 3: Representative image from ultrasound imaging system of sham and TAC mice after 4 weeks. (A) Pulsed-wave Doppler imaging of sham aortic arch. (B) Pulsed-wave Doppler imaging of aortic arch after TAC. (C) M-mode image of sham mouse calculating EF, LV Mass, wall thickness, and LVID. (D) M-mode image of TAC mouse calculating EF, LV Mass, wall thickness, and LVID. Please click here to view a larger version of this figure.
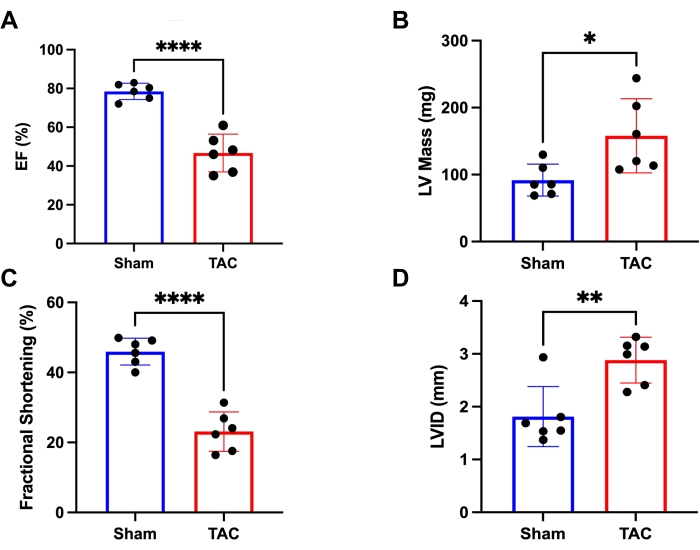
Figure 4: Heart function measured via Ultrasound Imaging System. (A) Ejection fraction (EF) of the mice in two groups. (B) The left ventricular mass (LV mass) of the mice was in two groups. (C) Fractional shortening (FS) of the mice in two groups. (D) The left ventricular internal diameter (LVID) of the mice in two groups. *p < 0.05, **p < 0.005, ***p < 0.0005. Data represents six mice per group. Please click here to view a larger version of this figure.
