In the initial experiments with this model, our group successfully achieved the desired outcome of a posterior cerebral or superior cerebellar artery occlusion in 12 out of 14 animals (85.7%). For the experiment, seven males and seven females were studied. The mean animal weight was 3.6 kg (± 0.46 kg). In the two animals in which success was not achieved, profound catheter-induced vasospasm precluded safe access to the intracranial circulation. In one rabbit, intracranial access could not be obtained due to occlusive vasospasm, and in the other animal, intracranial arterial perforation occurred during attempted catheterization, which was likely due to attempting to position the microcatheter too far distally in the posterior cerebral artery.
In all the animals, the brain was successfully harvested and subjected to histopathological analysis with either hematoxylin and eosin (H&E) staining or 2% triphenyltetrazolium chloride (TTC). In keeping with previously published results of the occlusion model, larger infarct volumes occurred with longer occlusion durations, which have been successfully performed from 60 to 240 min18. H&E stain images after 90 min of occlusion with 120 min of reperfusion are provided in Figure 3.
Baseline arterial BPs below normotension (40-60 mmHg systolic BP) were noted in all the animals after induction of anesthesia without use of vasopressors or inflation of an intra-aortic balloon. Partial inflation of the balloon has demonstrated immediate increase in systolic BP, with a sample BP tracing provided in Figure 4. This figure includes tracing of a short duration to visualize both the near-instantaneous change following inflation of the intra-aortic balloon as well as the changes throughout each cardiac cycle.
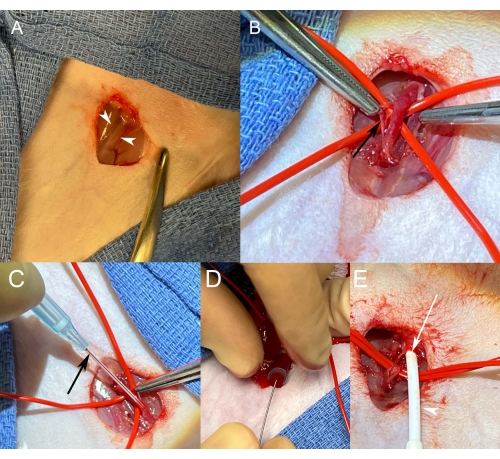
Figure 1: Femoral artery access. (A) Surgical exposure of the right femoral neurovascular bundle before blunt dissection. White arrowheads indicate the medial and lateral borders of the bundle to be exposed with dissection. (B) After isolation, the artery becomes engorged when dripping with lidocaine solution and applying gentle traction to the downstream vessel loop. The vessel can be cleaned by gentle dissection of tissue (black arrow) off the adventitia. (C) Maintaining gentle tension on the vessel, a 22 G angiocatheter is advanced into the vessel. After seeing blood flash in the angiocatheter (black arrow) and its chamber, the angiocatheter is gently advanced into the artery. (D) With the angiocatheter advanced in the artery to its hub, a Cope wire is advanced into the artery through the angiocatheter. (E) After removing the angiocatheter over a Cope microwire, a vascular sheath (white arrowhead) is advanced along with its inner introducer over the wire. The sheath is seen entering the artery, the wall of which can be seen at the arteriotomy site (white arrow). Please click here to view a larger version of this figure.
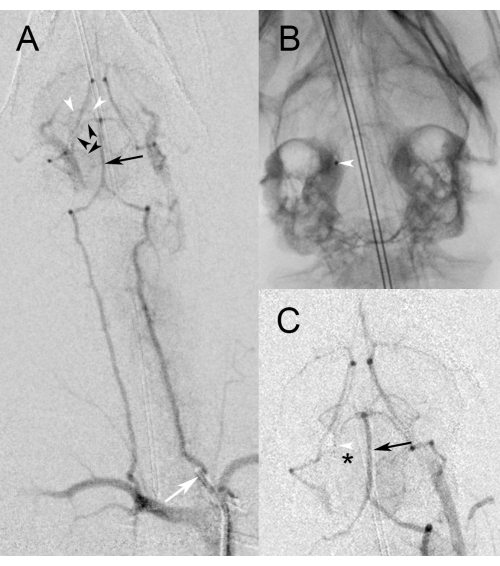
Figure 2: Angiographic images. (A) Low magnification view of digital subtraction angiography during injection of the proximal left vertebral artery (white arrow) demonstrates filling of the basilar artery (black arrow). Note the reflux back down the right vertebral artery into the subclavian artery, which can be used as a roadmap to guide catheterization. Black arrowheads delineate the course of the right superior cerebral artery that will be targeted for occlusion. White arrowheads identify the posterior cerebellar artery, which can also be targeted. (B) High magnification spot fluoroscopic image demonstrates the microcatheter in the right superior cerebellar artery from a right vertebral approach. The white arrowhead indicates the radiopaque marker at the microcatheter tip. (C) High magnification digital subtraction angiography during injection of the left vertebral artery demonstrates persistent filling of the basilar artery (black arrow) while the microcatheter runs through it. No filling is noted beyond the mid-right superior cerebellar artery, where the tip of the microcatheter is indicated by the white arrowhead. The black asterisk identifies non-perfused territory downstream to the occlusion in the superior cerebellar artery. Please click here to view a larger version of this figure.
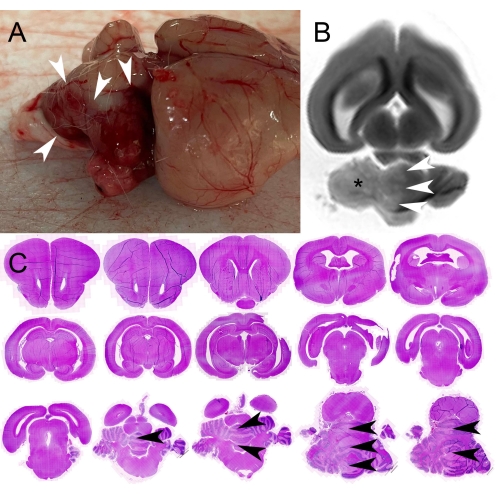
Figure 3: Pathology images. (A) Photograph of intact harvested brain showing the surface of the brain from the animal's right. Note the darkened appearance of the superior cerebellum indicating petechial hemorrhage in the acutely infarcted tissue. White arrowheads demarcate the margin of the infarction. (B) Long-axis T2-weighted magnetic resonance image of the intact brain in formalin. Note the increased signal in the right cerebellum (asterisk), consistent with the infarct, the border of which is delineated by white arrowheads. (C) Bright field images of 1.5 mm thick serial coronal sections following hematoxylin and eosin (H&E) staining demonstrates infarction in the right cerebellum, the margin of which is indicated by black arrowheads on multiple slices. These sections were sliced from blocks of a harvested rabbit brain cut in the coronal plane with a cutting matrix. Please click here to view a larger version of this figure.
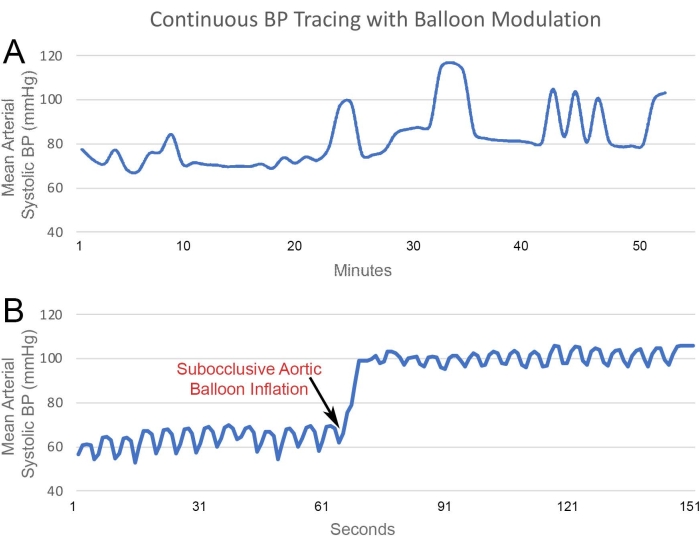
Figure 4: BP Monitoring. BP pressure tracing from a Fogarty balloon catheter positioned in the infrarenal aorta. (A) Data from approximately 1 h of BP monitoring demonstrates real-time arterial pressure changes with changes in balloon inflation. (B) Short-term tracing demonstrates the pressure changes throughout the cardiac cycle. Additionally, small, rapid changes are noted from respiratory variability, which is physiologically normal. An immediate near-doubling of measured BP is noted following the inflation of the balloon. Please click here to view a larger version of this figure.
