Tumor size declines in animals treated with SDT 24 h post-treatment.
On the day of SDT treatment, the original average bioluminescence signal for the control and treatment groups (N = 4 each) was 2.0 x 106 ± 3.1 x 106 and 2.3 x 106 ± 1.3 x 106 p/s/cm2/sr, respectively. The average bioluminescence values corresponding to tumor size before treatment between the two groups were not statistically significant (p = 0.89). The average bioluminescence signal of the treatment group was 3.57 x 106 ± 2.3 x 106 24 h following SDT, while the bioluminescent signal of the control group was increased to 5.5 x 106 ± 8.2 x 106 p/s/cm2/sr. As shown in Figure 5, this corresponds to a growth rate of 83.4% ± 78% and 172% ± 34%, respectively, assuming exponential growth (p = 0.08). Of the four treated animals, three had lower growth rates post-treatment compared to controls. There was one outlier in the treatment group that showed comparable growth to controls, skewing the deviations.
Additionally, the animals underwent subsequent contrast-enhanced MR imaging the day following treatment for pre- and post-treatment comparison of the tumor. The average grayscale intensity of contrast agent in tumors was conducted across each MRI slice for each animal to measure how much contrast agent was entering tumors following treatment, as an estimate of tumor size. Pre-treatment, the average tumor grayscale intensity between control and treated groups was similar. On average, this greyscale intensity increased in the control group to a larger magnitude than in treated groups, although this was not significant (p = 0.47). This data can be seen in Table 2. The high variability of these results is potentially due to the fact that MRIs were taken only 24 h post-treatment, at which time the therapeutic potential of SDT is only beginning to occur. Even so, Figure 6 shows an example of the lesions created by SDT.
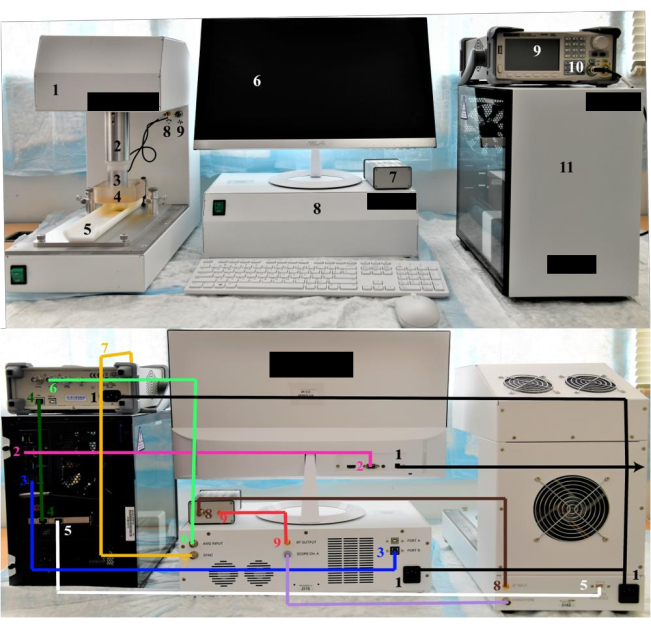
Figure 1: FUS system setup. (Top) MRgFUS System with labeled components. (Front) 1. Platform. 2. Axis motorized transducer arm. 3. FUS transducer. 4. Water bath. 5. MRI bed. 6. Monitor. 7. Transducer impedance matching box. 8. Power amplifier box. 9. Function generator. 10. Function generator channel 1 BNC port. 11. Desktop computer. (Bottom) MRgFUS system with color-coded wiring schematic with the following connections. (Back) 1. Power cords. 2. Monitor HDMI to desktop HDMI. 3. Port B USB B to desktop USB A. 4. Oscilloscope LAN ethernet to desktop ethernet. 5. Motion interface ethernet to desktop ethernet. 6. Oscilloscope aux in/out BNC to AWG input BNC. 7. Oscilloscope channel 1 (Front) BNC to SYNC BNC. 8. Matching box output BNC to RF input coaxial. 9. RF output coaxial to matching box coaxial. Please click here to view a larger version of this figure.
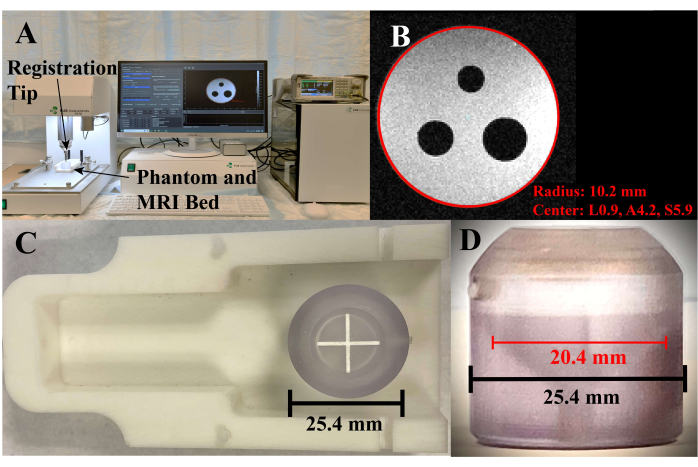
Figure 2: Phantom registration. (A) System setup and software during phantom registration. (B) Screenshot of the phantom registration screen, where the red circle is the selected circumference of the axial cross section. (C) Phantom placed on the MRI bed, top view. (D) Side view of the phantom, where the red line is in the axial slice corresponding to the circle in C. Please click here to view a larger version of this figure.
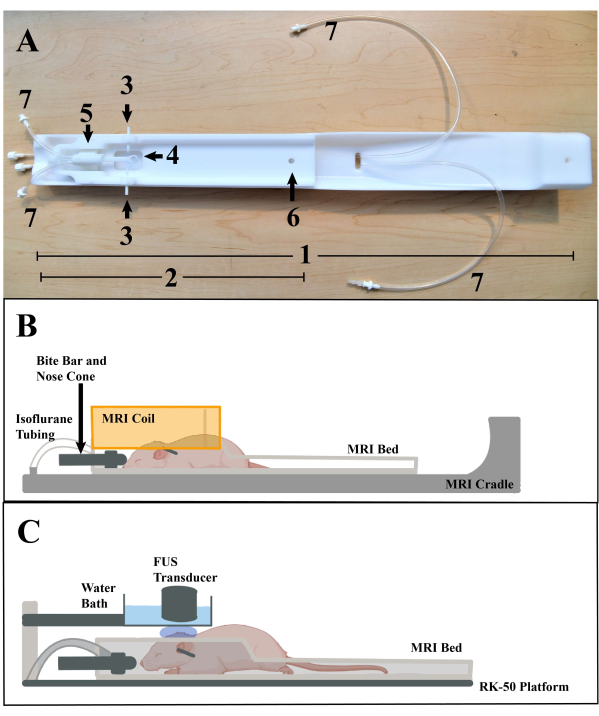
Figure 3: Animal placement. (A) MRI bed and cradle, with various parts labeled: 1. MRI cradle. 2. Stereotactic MRI bed. 3. Ear bars. 4. Bite bar. 5. Nose cone. 6. MRI bed peg hole. 7. Isoflurane anesthesia tubes. (B) Illustration representing the placement of the mouse on the MRI bed and placement on the cradle, with the RF coil (Orange) (illustration modified using Biorender 2022 template). (C) Illustration representing the placement of the mouse on the MRI bed during a FUS treatment (illustration modified using Biorender 2022 template). Please click here to view a larger version of this figure.
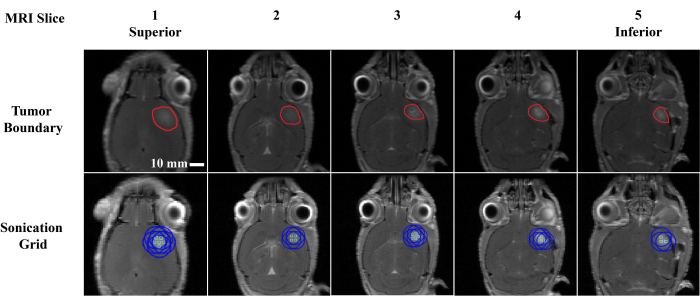
Figure 4: Focal point selection. Example of a sonication point selection in a single animal. Each column represents a T1-weighted post-contrast MRI slice where each slice is 0.5 mm in the proximal (slice 1) to distal (slice 5) direction. The tumor boundary was manually segmented and is outlined in red (row 1), and the corresponding sonication locations (row 2) are represented by a light green square (focal max center) and blue circle (half max focal circumference). Each location was sonicated for 2 min. Please click here to view a larger version of this figure.
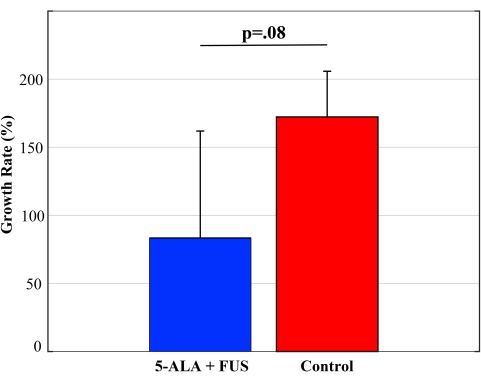
Figure 5: Growth rate following SDT. The growth rate of GBM tumors from pre- to 24 h post-SDT treatment in treated and untreated (control) animals with intracranial M59 tumors based on the measured luminescence. Error bars indicate standard deviation. A two-sample student's T-test was performed to determine significance. Please click here to view a larger version of this figure.
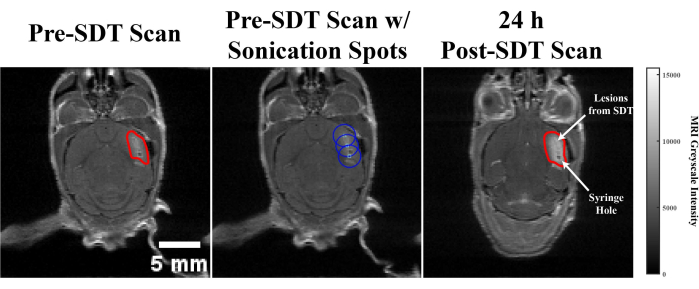
Figure 6: SDT generated lesion. Pre- and post-contrast enhance T1-weighted MRI scans from an animal model featuring a representative axial slice showing a lesion in the tumor created by SDT. (Left) MRI scan taken prior to SDT treatment, with the tumor outlined in red. (Middle) FUS focal point selection where the maximum pressure is represented by light blue circles and the half-maximum pressure regions are represented by blue circles. (Right) Post-SDT MRI scans, where the tumor is outlined in red. SDT-created lesions and the syringe hole for implantation are shown. Please click here to view a larger version of this figure.
| Sequence | T1 |
| Repetition time | 3000 ms |
| Echo time | 30 ms |
| Slice thickness | 0.5 mm |
| Number of slices | 25 |
| Pixel spacing | 0.187 mm x 0.187 mm |
| Acquisition matrix | 133 x 133 |
| Averages | 4 |
Table 1: MRI settings.
| Control | SDT Group | P-Value | |
| Pre-Treatment | 7.49 x 103 ± 2.2 x 103 | 7.48 x 103 ± 1 x 103 | 0.99 |
| Post-Treatment | 8.79 x 103 ± 7.7 x 102 | 7.95 x 103 ± 1.1 x 103 | 0.33 |
| Percent Difference | 16% ± 16% | 7% ± 12% | 0.47 |
Table 2: Post-contrast enhanced T1-weighted MRI greyscale.
