The C. albicans and biofilms on the catheters could be observed by the SEM. As shown in Figure 322, the surface of the polyethylene catheters in the catheter group was smooth, and no adhered pathogenic microorganism was observed. However, mature and dense C. albicans biofilms were visible on the surface of the polyethylene catheters in the model group, indicating that C. albicans could successfully colonize and form biofilms on the catheter surface in mice under the experimental conditions. Moreover, fluorescence microscopy results further verified the above conclusions (Figure 4)22. There was no obvious fluorescence on the surface of the polyethylene catheters in the catheter group. However, strong fluorescence emitted by adherent C. albicans cells was visible on the catheter surface in the model group. This indicated that a large number of C. albicans cells adhered to the surface of the catheters, which demonstrated the successful construction of C. albicans biofilm-related CRI models in mice.
In order to verify the infection of mouse skin tissue more intuitively, Sheff Periodate staining analysis was performed. It detects the carbohydrates of the fungal cells, which is commonly used in clinical research (Figure 5)22. The skin tissue in the normal control and catheter group was stained negatively by periodic acid-Schiff (PAS), which indicated the absence of C. albicans cells in the tissues. A small number of positive PAS-stained C. albicans cells were observed in the model group, further validating the successful simulation of C. albicans-related invasion and adhesion.
Next, the pathological changes in mice skin tissues induced by C. albicans were evaluated by histopathological analysis. As shown in Figure 622, the epidermis layer was significantly thickened and extended to the inner part of the skin in the model group. Inflammation infiltration was also visible, indicating that the infection of C. albicans caused obvious pathological changes in mouse skin tissue. The epidermis layer, dermis layer, sebaceous glands, hair follicles, and other structures were clear and complete in the catheter group. No edema and inflammation infiltration were observed, similar to the normal control group. These results indicated that inserting the catheter alone did not cause obvious changes in the skin tissue. The pathological changes in the tissues of the model group resulted from the infection caused by C. albicans. In summary, the results validate the successful establishment of a CRI mouse model associated with C. albicans biofilm.
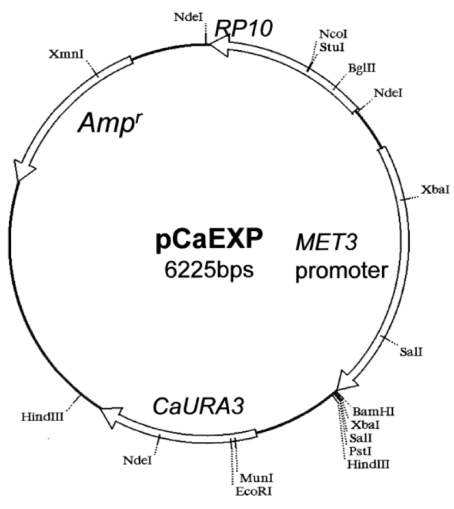
Figure 1: pCaExp plasmid atlas. Please click here to view a larger version of this figure.
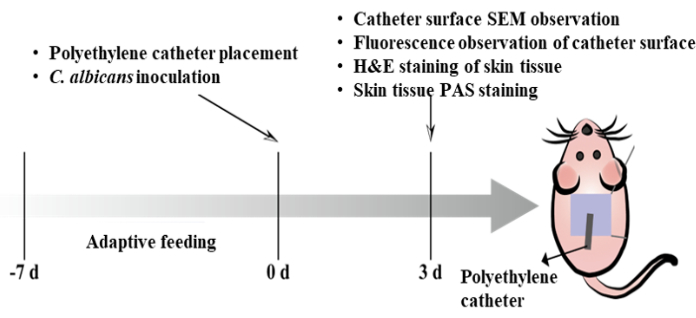
Figure 2: Schematic showing the procedure of the C.albicans-associated CRI mice model. Please click here to view a larger version of this figure.
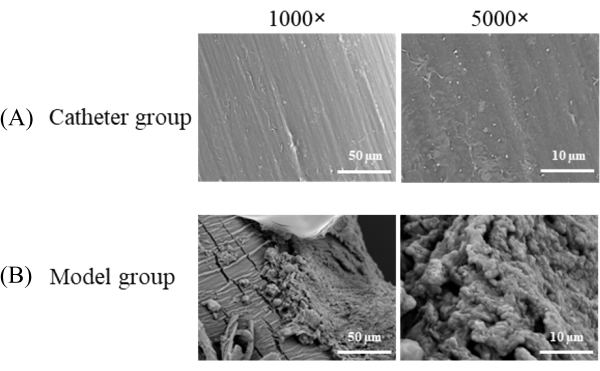
Figure 3: SEM on the surface of the catheter in each group. (A) Catheter group; (B) Model group (1000x, scale bar = 50 µm; 5000x, scale bar = 10 µm). This figure has been modified with permission from Mo et al.22. Please click here to view a larger version of this figure.
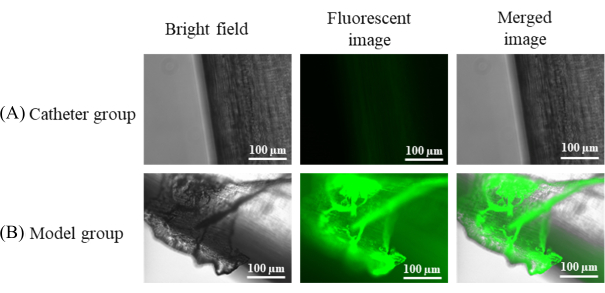
Figure 4: Catheter surface fluorescence microscopy in each group. (A) Catheter group; (B) Model group (scale bar = 100 µm). This figure has been modified with permission from Mo et al.22. Please click here to view a larger version of this figure.
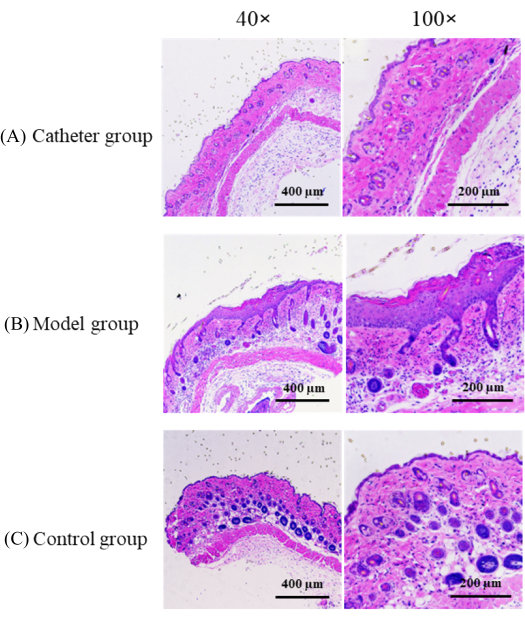
Figure 5: H&E staining of the back skin of mice in each group. (A) Catheter group; (B) Model group; (C) Control group, (40x, scale bar = 400 µm; 100x, scale bar = 200 µm). This figure has been modified with permission from Mo et al.22. Please click here to view a larger version of this figure.
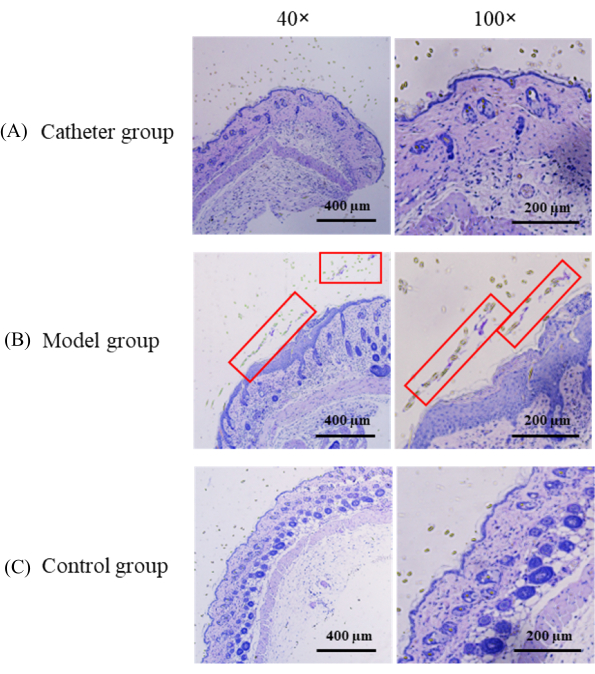
Figure 6: PAS staining of the back skin of mice in each group. (A) Catheter group; (B) Model group; (C) Control group, (40x, scale bar = 400 µm; 100x, scale bar = 200 µm). Significant thickening and extension of the epidermis layer to the inner part of the skin can be seen in the model group (red rectangles). This figure has been modified with permission from Mo et al.22. Please click here to view a larger version of this figure.
