To validate whether patient assessments of desquamation, erythema, and induration are comparable to those of a dermatologist, 27 psoriasis patients at the University of Utah dermatology clinic were enlisted to complete a questionnaire about psoriasis severity at the time of the questionnaire's administration. Each participant was provided with a Psoriasis Thickness Reference Card along with the questionnaire. The dermatologist provided their independent assessment of the current status of each patient using the same measuring scales.
Psoriasis severity was categorized into two groups, mild versus moderate to severe. Grouping moderate and severe psoriasis aligns with the clinical management of psoriasis patients. For induration, moderate corresponds to 5-8 sticky notes and severe corresponds to 10-13 sticky notes. The accuracy of patients' assessments of desquamation, erythema, and induration was evaluated by sensitivity (the test's ability to correctly identify an individual as having the disease) and specificity (the test's ability to correctly identify an individual as not having the disease) using the physician's assessments as the gold standard. The Wilcoxon signed-rank test was used to examine whether patient assessments of psoriasis severity differed significantly from those of the attending dermatologist. Cohen's kappa was used to evaluate whether the two assessments were comparable.
The results demonstrated that the patients' and physician's answers to some questions regarding psoriasis severity are moderately to highly concordant (Figure 2 and Table 1). The numbers of physician-patient severity assessments with matching values were 23 (85.2%), 25 (92.6%), and 22 (84.6%) for desquamation, erythema, and induration (which was answered by 26 out of 27 participants), respectively. There was no significant difference between patient and physician reports of desquamation (p = 0.42), erythema (p > 0.99), and induration (p > 0.99) by the Wilcoxon signed-rank test. Sensitivity ranged from 0.83 to 0.93 and specificity from 0.77 to 0.92. Cohen's kappa values revealed at least some level of agreement between the physician and patient assessments of all three variables (kappa scores > 0.69, p-values < 0.000002). Using Cohen's kappa interpretations suggested by McHugh13, moderate agreement was observed between physician and patient measurements of desquamation and induration; physician and patient measurements of erythema exhibited strong agreement.
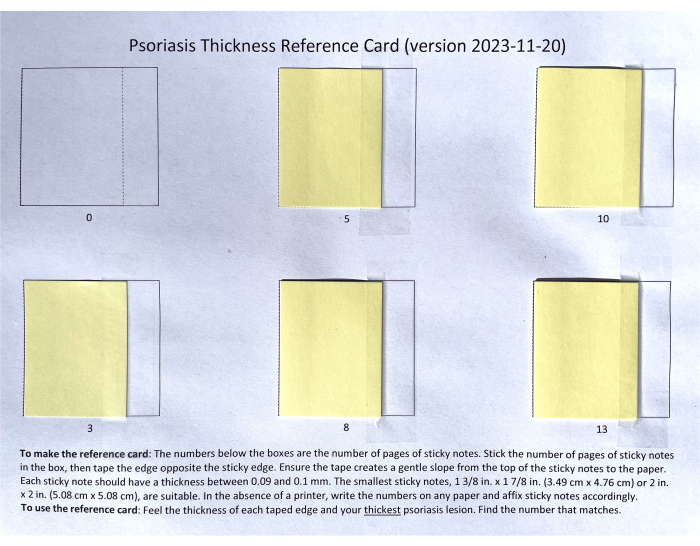
Figure 1: Completed Psoriasis Thickness Reference Card. The number under each square in the card indicates the number of sticky notes in each stack. The stacks of sticky notes are attached to the paper using the adhesive side of the notes on the left and a piece of tape on the right. Please click here to view a larger version of this figure.
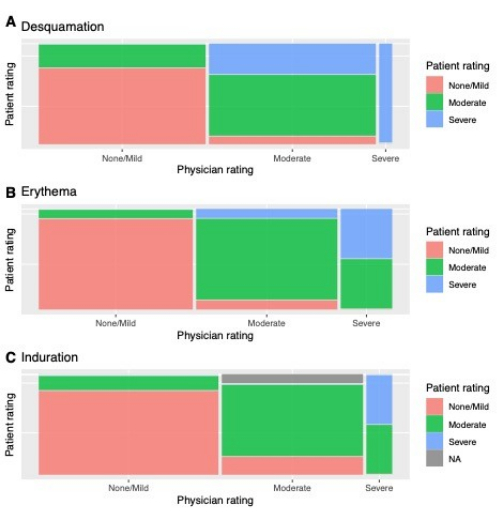
Figure 2: Proportions of patient assessments that matched or did not match physician assessments. Each patient rated the severity of their current psoriasis lesions based on three psoriatic features; the attending dermatologist also rated each patient's psoriasis severity on the same scale. Each of the three columns represents physician ratings; the width of each column represents the proportion of patients given that rating by the physician. Within each column, the different colors represent the proportion of those patients given a specific physician rating who were also given a specific patient rating, e.g. approximately 50% of the patients who were assessed as having severe erythema by a physician were self-assessed as having moderate erythema. (A) Desquamation, (B) erythema, and (C) induration. Abbreviation: NA = not applicable (patient did not provide an assessment). Please click here to view a larger version of this figure.
| Desquamation | Erythema | Induration | |
| True positive* | 13 | 14 | 10 |
| False positive* | 3 | 1 | 2 |
| False negative* | 1 | 1 | 2 |
| True negative* | 10 | 11 | 12 |
| Sensitivity | 0.93 | 0.93 | 0.83 |
| Specificity | 0.77 | 0.92 | 0.86 |
| Accuracy | 0.85 | 0.93 | 0.85 |
| Wilcoxon signed rank test p-value | 0.42 | >0.99 | >0.99 |
| Cohen’s kappa value [95% CI] | 0.70 [0.43,0.97] | 0.85 [0.65,1.00] | 0.69 [0.41,0.97] |
| Cohen’s kappa category | Moderate | Strong | Moderate |
Table 1: Predictive value, sensitivity, and specificity of patient psoriasis severity ratings. Physician ratings were treated as the true values to which the patient ratings were compared. *Positive is moderate to severe psoriasis; negative is mild to no psoriasis. Abbreviation: CI = confidence interval.
Supplemental Figure S1: Psoriasis thickness Reference Card template. The template may be printed and used to directly place the sticky notes on, or it may be used as a guide for numbering and placing sticky notes on a sheet of paper if no printer is available. Please click here to download this File.
