The surgery proceeded smoothly, and the intraoperative rapid frozen pathological examination indicated the absence of cancer at the incisal margin of the pancreas. Throughout the surgery, the patient's vital signs remained stable, and the anesthesia was effective. The operation duration was 150 min, with an intraoperative blood loss of 80 mL. Anal exhaust occurred 32 h postoperatively. There were no complications such as abdominal hemorrhage, pancreatic leakage, abdominal infection, or incision infection. The postoperative hospital stay was 6 days.
The histopathological analysis of postoperative paraffin sections revealed moderately differentiated pancreatic ductal adenocarcinoma (Figure 10). No tumor tissues were identified at the incisal margin of the pancreas. Fourteen lymph nodes were removed, and one exhibited metastasis. The tumor stage was determined to be pT3N1M0, IIB (Table 1). A postoperative CT scan demonstrated the successful removal of the tumor without significant recurrence or metastasis (Figure 11).
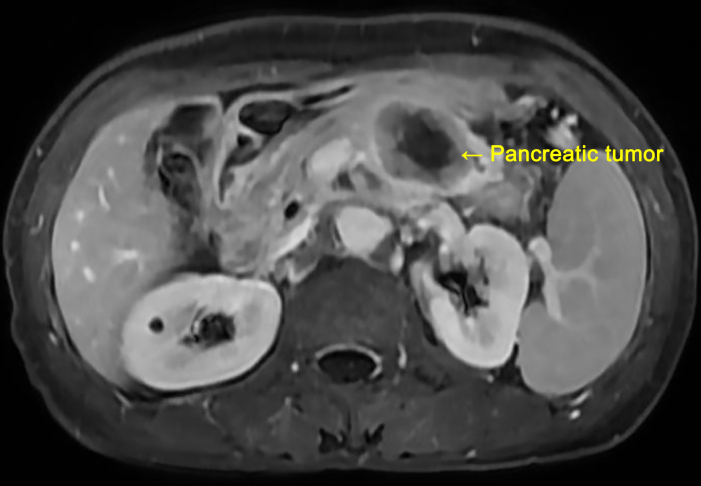
Figure 1: Presurgical abdominal MRI image of the patient. The abdominal MRI indicates that the size of the pancreatic body and tail mass is approximately 3.5 cm × 3.0 cm × 3.0 cm, suggesting an epithelial-derived malignant tumor. Please click here to view a larger version of this figure.
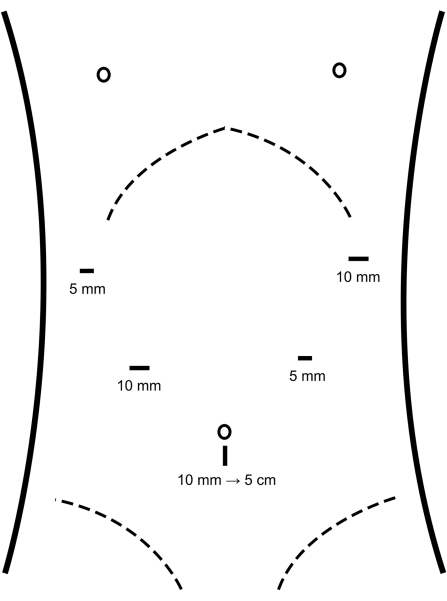
Figure 2: Location of the trocars. Trocars are placed into the abdominal cavity at the locations depicted in the figure. Please click here to view a larger version of this figure.
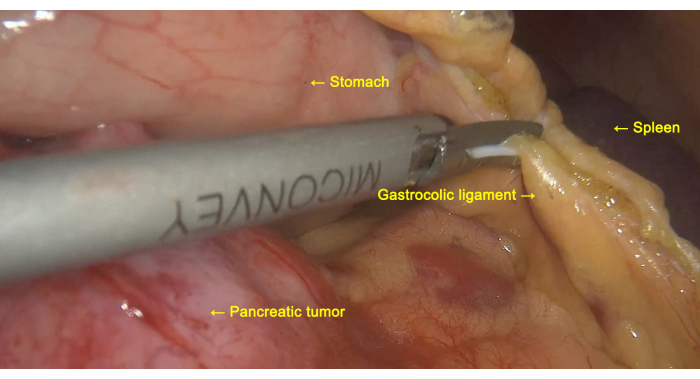
Figure 3: Exploration of the pancreatic tumor. The gastrocolic ligament is cut to facilitate the exploration of the pancreatic tumor. Please click here to view a larger version of this figure.
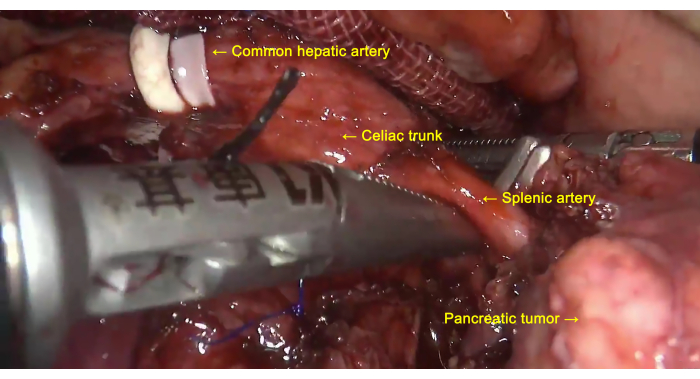
Figure 4: Lymph node dissection. Lymph nodes around the common hepatic artery, celiac trunk, and splenic artery are dissected. Please click here to view a larger version of this figure.
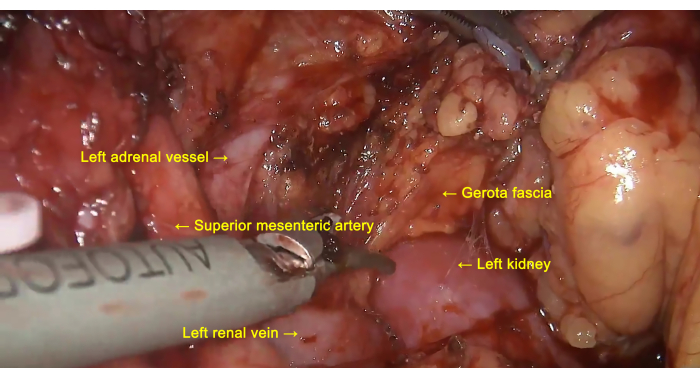
Figure 5: Removal of the anterior layer of Gerota fascia. Lymph nodes around the superior mesenteric artery (SMA) are dissected, and the anterior layer of Gerota fascia is peeled from the surface of the left kidney along the left renal vein. Please click here to view a larger version of this figure.
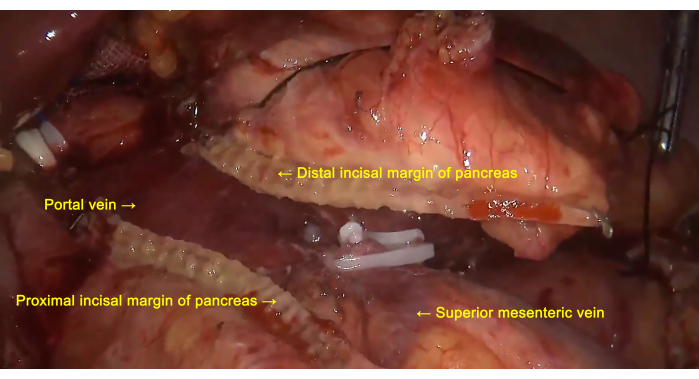
Figure 6: Pancreatic transection. The pancreas is severed at the neck using a linear stapling device. Please click here to view a larger version of this figure.
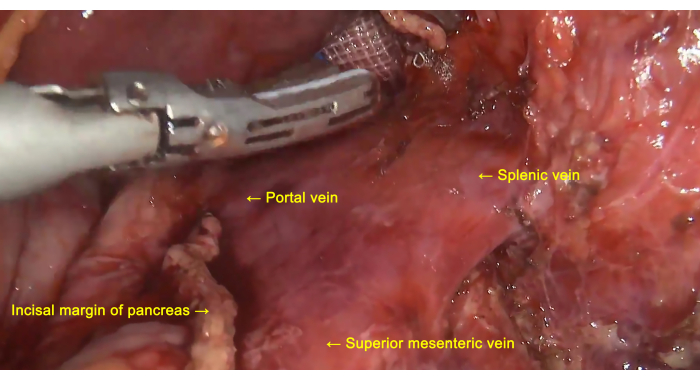
Figure 7: Treatment of the splenic vein. The splenic vein is dissected, exposed, ligated, and severed at the root. Please click here to view a larger version of this figure.
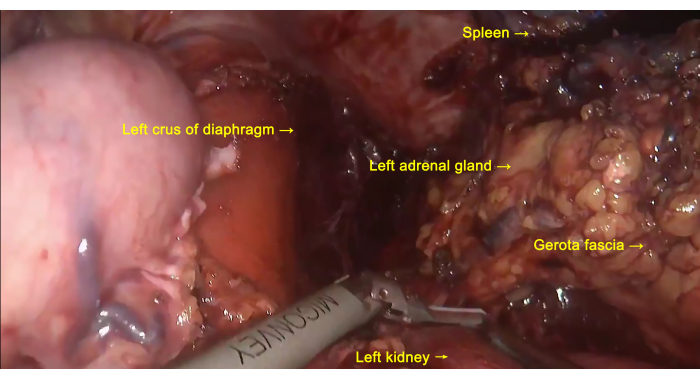
Figure 8: En Bloc resection. The distal pancreas, the anterior layer of Gerota fascia, the left adrenal gland, and the spleen are removed as a single entity. Please click here to view a larger version of this figure.
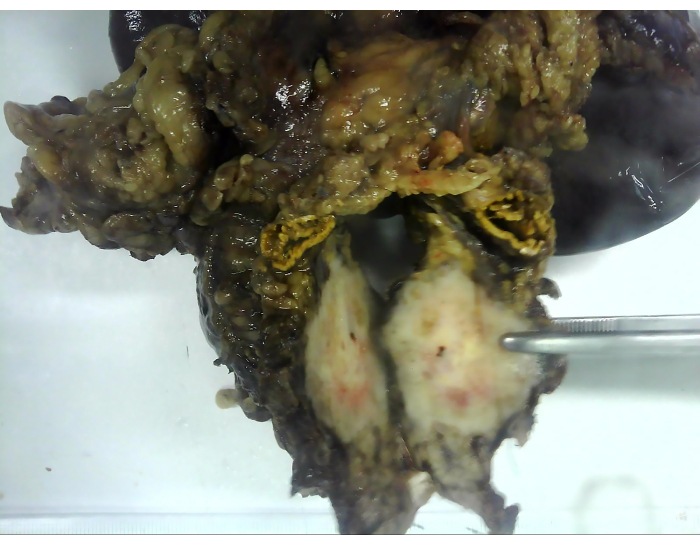
Figure 9: The excised specimen. The excised specimen includes the distal pancreas, the anterior layer of Gerota fascia, the left adrenal gland, and the spleen. Please click here to view a larger version of this figure.
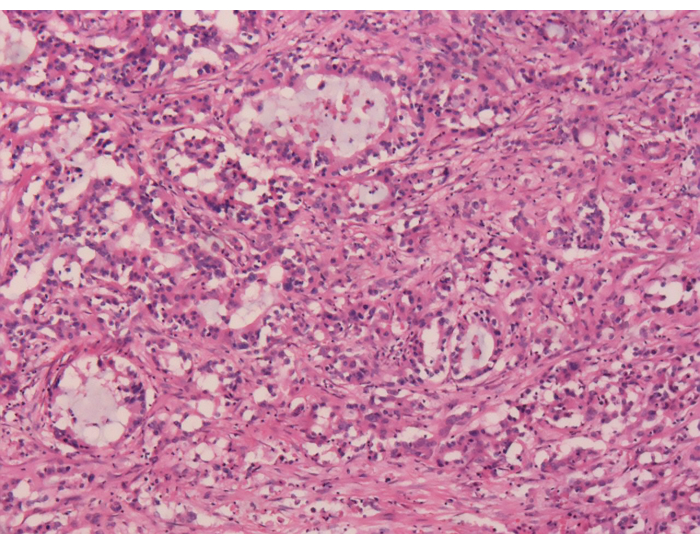
Figure 10: Postoperative histopathological examination. Postoperative paraffin sections reveal moderately differentiated pancreatic ductal adenocarcinoma. Magnification: 40x. Please click here to view a larger version of this figure.
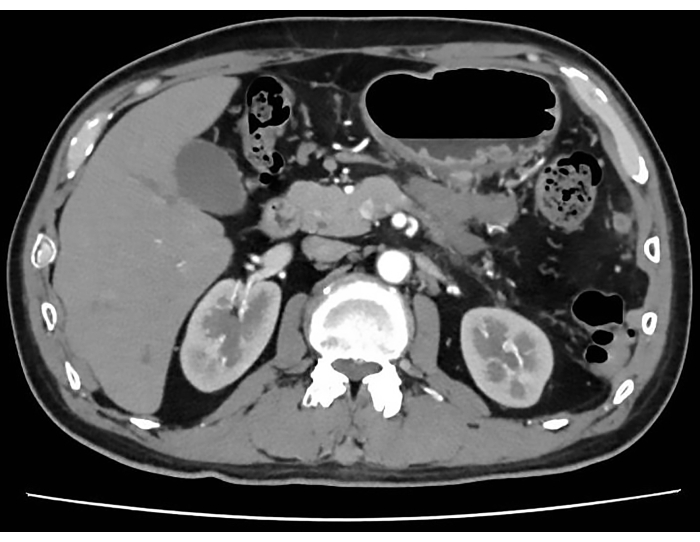
Figure 11: Postoperative CT scan. The postoperative CT scan indicates successful tumor removal without significant recurrence or metastasis. Please click here to view a larger version of this figure.
| Operation time (min) | 150 |
| Intraoperative blood loss (mL) | 80 |
| First flatus (h) | 32 |
| First postoperative liquid diet (days) | 1 |
| Postoperative hospital stay (days) | 6 |
| Postoperative complications (yes/no) | no |
| Bleeding (yes/no) | no |
| Pancreatic leakage (yes/no) | no |
| Abdominal infection (yes/no) | no |
| Incision infection (yes/no) | no |
| Pathological result | Pancreatic ductal adenocarcinoma |
| Differentiation | Moderate |
| TNM stage | pT3N1M0 |
| AJCC stage | IIB |
Table 1: The surgical outcomes of the patient.
