Figure 1A,B illustrate HR-OCT images of OSSN, revealing three key characteristics: (1) Significantly thickened hyper-reflective epithelium; (2) An abrupt shift from normal to abnormal epithelium, marked by a sudden rise in both brightness and thickness of the epithelium; (3) Occasionally, a division plane is visible between the epithelium and underlying tissue. However, in very thick lesions, the lower edge of the lesion may be somewhat obscured by shadowing.
The sub-epithelial tissue is usually of normal thickness in simple OSSN lesions. However, unlike OSSN, the HR-OCT findings of other ocular lesions like pterygia, pseudopterygium, and dermoid often reveal normal to slightly thickened epithelium accompanied by dense, hyperreflective thickened subepithelial mass (Figure 1C–H). The corneal epithelium is usually dark and thin, while that of the conjunctiva is thin but mildly hyper-reflective and sometimes intense as well, which may be caused by actinic changes. These unique characteristics were always parallel to the changes seen on histopathologic examination, which makes HR-OCT an important modality for differentiating OSSN from various ocular surface pathologies8.
HR-OCT can also be used to monitor the chemotherapeutic response of OSSN. During topical chemotherapeutic treatment, a decrease in epithelial thickness and hyperreflectivity can be seen after 2 cycles of topical chemotherapy, which indicates the time point of clinical regression of OSSN, which can help clinicians determine the therapy duration (Figure 2). In addition, the restoration of normal anatomy can also be detected during follow-up visits.
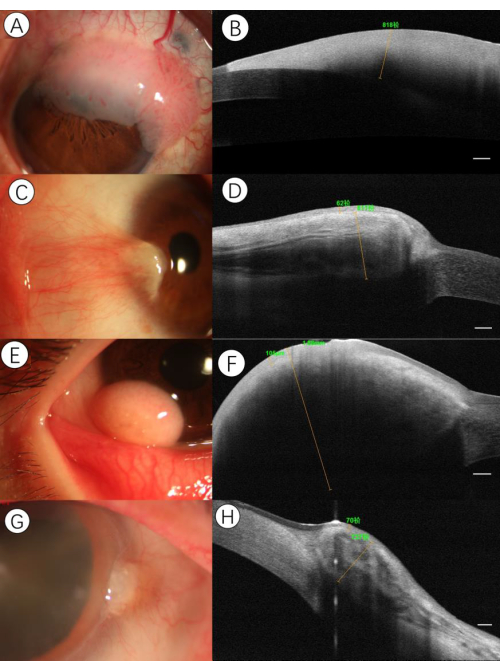
Figure 1: Sample imaging of various ocular surface lesions. (A) Slit-lamp photograph demonstrating gelatinous OSSN. A 58-year-old male presented with a limbal lesion in the upper quadrant of the left eye. (B) HR-OCT disclosed a well-circumscribed, severely hyper-reflective epithelium with a shadowing effect. An abrupt transition between normal and thickened hyperreflective epithelium could be seen, as well as a plane of cleavage between the lesion and the underlying tissue. The maximal epithelial thickness value of the lesion was over 818 µm. (C) Slit-lamp photograph demonstrating pterygia. A 36-year-old female presented with a conjunctival and corneal lesion consistent with pterygium. (D) HR-OCT disclosed a thickened sub-epithelial lesion with a striped reflection, which likely corresponded to the vasculature and the overlying thin epithelium separated by a plane of cleavage. The maximal epithelial and sub-epithelial thickness values of the lesion were 62 µm and 811 µm, respectively. (E) Slit-lamp photograph demonstrating lipodermoid. A 13-year-old male presented with an adipose-like lesion in the nasal quadrant of the left eye. (F) HR-OCT disclosed a thin epithelium with an underlying severely thickened uniformed tissue with shadowing. The maximal epithelial and sub-epithelial thickness values of the lesion were 105 µm and 1.88 mm, respectively. (G) Slit-lamp photograph demonstrating pseudopterygium. A 70-year-old female presented with a raised conjunctival lesion at the limbus in the nasal portion of the right eye. (H) HR-OCT disclosed a moderately hyperreflective epithelium with a thickened lesion in the substantia propria intermixed with a hyporeflective cluster area. The maximal epithelial and sub-epithelial thickness values of the lesion were 70 µm and 737 µm, respectively. Scale bars: 250µm. Please click here to view a larger version of this figure.
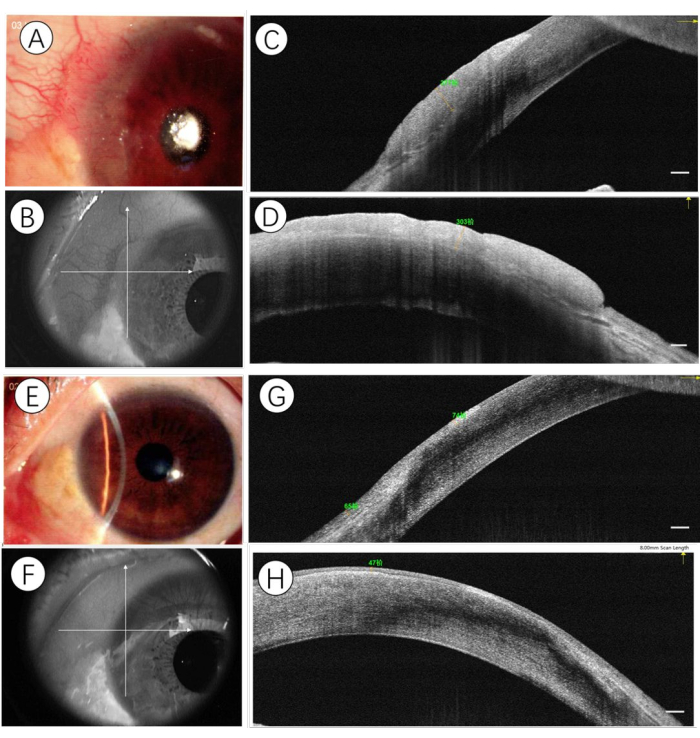
Figure 2: Sample imaging of OSSN before and after topical chemotherapy. (A) At presentation, a slit-lamp photograph demonstrating a gelatinous OSSN. The cross line is aligned to the center of the lesion (B), and HR-OCT identified the horizontal (C) and vertical (D) expanse of the lesion of a hyper-reflective thickened epithelium. After a 2-month basis of topical chemotherapy (5-fluorouracil 1%, one week-on, 3 weeks-off, given four times daily; Interferon-α2b 1MIU/mL, given four times daily), the slit-lamp photograph demonstrated a complete resolution of the lesion (E). The cross line is aligned to the original spot (F), and HR-OCT identified the horizontal (G) and vertical (H) expanse of a hyper-reflective epithelium in normal thickness. Scale bars: 250µm. Please click here to view a larger version of this figure.
