In this study, 7 individuals failed to complete the trial. All necessary data were gathered from 83 individuals who completed the trial. There were 38 women and 45 men. The age ranged from 44 to 75 years old, with an average age of (60.57 + 8.76). DM might last anywhere between 4 and 22 years, with an average of 14.10 + 4.85 years. DPN lasted anywhere from one and fifteen years, with a mean of 5.76 + 2.78 years. The general data of the three groups did not differ significantly (p>0.05).
After the intervention, there was a statistically significant difference in the TCSS scores of the three groups (P < 0.001) (see Table 2). Further multiple comparisons showed that the TCSS score of the MTCG was significantly lower than that of the TCG and lower than the CG, and the difference was statistically significant (P < 0.05) (see Figure 1). These results revealed that the neurological symptoms improved after the intervention.
After the intervention, the MAAS scores of the three groups were significantly different (P < 0.05) (see Table 2). Further multiple comparisons showed no significant difference in the MAAS scores between the CG and the TCG (P > 0.05). The MAAS score of MTCG was significantly higher than that of TCG and CG (P < 0.05) (see Figure 2). The MAAS score revealed that mindfulness training combined with Taijiquan could improve the subjects' mindfulness levels. At the same time, it shows that the improvement of the exercise effect may be related to the improvement of mindfulness level.
After the intervention, there was a statistically significant difference in the VAS score between the three groups (P < 0.05) (see Table 3). Further multiple comparisons showed that the pain relief effect of mindfulness combined with MTCG was significantly better than that of TCG and CG, and the difference was statistically significant (P<0.05). (see Figure 3)
After the intervention, there was a statistically significant difference in the levels of TNF-α among the three groups (P < 0.05) (see Table 3). Further multiple comparisons showed that the level of serum TNF-α in the MTCG was significantly lower than that in the TCG and lower than that in the CG, and the difference was statistically significant (P < 0.05). (see Figure 4)
After the intervention, there was a statistically significant difference in the DSQL scores (P<0.05) (see Table 4). Further multiple comparisons showed that the DSQL score of the CG was significantly lower than that of the TCG and lower than the MTCG, and the difference was statistically significant (P < 0.05) (see Figure 5). This suggests that mindfulness training combined with Tai Chi can significantly improve the quality of life of patients with DPN.
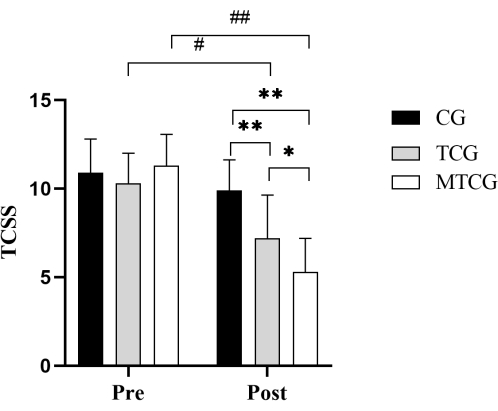
Figure 1: Comparison of TCSS scores among the three groups. **P < 0.01 intergroup comparisons, *P < 0.05 intergroup comparisons, ##P < 0.01 within-group comparisons, #P < 0.01 within-group comparisons. TCSS, Toronto Clinical Scoring System; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with Tai Chi group. Please click here to view a larger version of this figure.
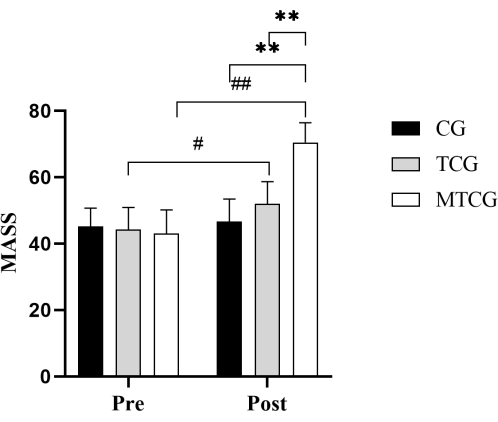
Figure 2. Comparison of MASS scores among the three groups.**P < 0.01 intergroup comparisons, ##P < 0.01 within-group comparisons, and #P < 0.01 within-group comparisons. MAAS, Mindful Attention Awareness Scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with Tai Chi group. Please click here to view a larger version of this figure.
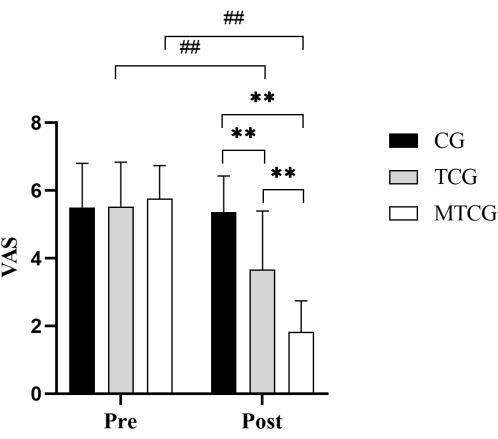
Figure 3. Comparison of VAS scores among the three groups. **P < 0.01 intergroup comparisons, and ##P < 0.01 within-group comparisons. VAS, Visual analog scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with Tai Chi group. Please click here to view a larger version of this figure.
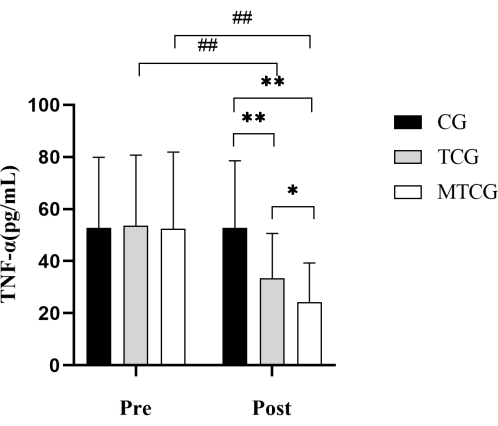
Figure 4. Comparison of serum TNF- α level among the three groups. **P < 0.01 intergroup comparisons, *P < 0.01 intergroup comparisons, and ##P < 0.01 within-group comparisons. TNF-α, Serum tumor necrosis factor-α; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with Tai Chi group. Please click here to view a larger version of this figure.
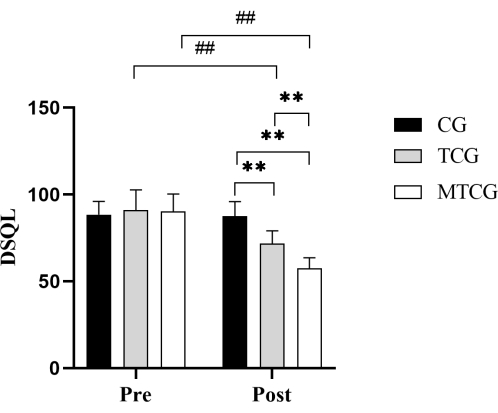
Figure 5. Comparison of DSQL scores among the three groups. **P < 0.01 intergroup comparisons, ##P < 0.01 within-group comparisons. DSQL, Diabetes Specificity Quality of life Scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with Tai Chi group. Please click here to view a larger version of this figure.
Table 1: Mindfulness training combined with Tai Chi training program schedule. Please click here to download this Table.
Table 2: Comparison of TCSS and MAAS and scores among the three groups. TCSS, Toronto Clinical Scoring System; MAAS, Mindful Attention Awareness Scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with the Tai Chi group. Please click here to download this Table.
Table 3: Comparison of VAS scores and TNF-α among the three groups. VAS, Visual analog scale; TNF-α, Serum tumor necrosis factor-α; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with the Tai Chi group. DSQL, Diabetes Specificity Quality of Life Scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with the Tai Chi group. Please click here to download this Table.
Table 4: Comparison of DSQL scores among the three groups. DSQL, Diabetes Specificity Quality of Life Scale; CG, the control group; TCG, the Tai Chi group; MTCG, the mindfulness training combined with the Tai Chi group. Please click here to download this Table.
