Here we described the integration process of CBCT and DDI using an AI-based program. To evaluate its reliability and reproducibility, a comparative study with surface-based registration (SBR) was conducted. It was determined that a minimum sample size of ten was required after a power analysis under correlation ρ H1 = 0.77, α = 0.05, and power (1−β) = 0.8018. A total of 17 sets of CBCT scans and digital dental images from orthognathic patients at Seoul National University Bundang Hospital from March 2016 to October 2019 were studied. The entire SBR and ABR processes for the same population were repeated twice by the same examiner, an orthodontic resident who had trained in landmark identification for more than 1.5 years. SBR was performed through a protocol similar to that of some previous studies9,10 (Figure 10). The mean differences in x, y, and z coordinate values of R-/L-U6CP, and R U1CP after repeated integrations with each program were evaluated. All data were statistically analyzed with SPSS 22.0 software. Reliability in the coordinates of the landmarks was analyzed in each ABR, SBR, and between them to evaluate reproducibility using intraclass correlation (ICC)19.
The intra-observer reliability of x-, y-, and z-coordinate values of R-/L-U6CP, and R U1CP was significant and almost perfect for ABR (0.950 ≤ ICC ≤ 0.998) and SBR (0.886 ≤ ICC ≤ 0.997), respectively (Table 1). The reliability difference in the y- and z-coordinate values in most landmarks was significant and showed almost perfect to substantial agreement between the SBR and ABR. However, the x-coordinate values of R-/L-U6CP and R U1CP presented moderate, mediocre, and low agreement, respectively, and were insignificant.
As shown in Table 2, the mean differences of all coordinate values from the repeated integrations were not significantly different in each method. These differences on the x-coordinates ranged from -0.005 to -0.098 mm for ABR and from -0.212 to 0.013 mm for SBR. They ranged from -0.084 to -0.314 mm on the y-coordinates for ABR, and from−0.007 to 0.084 mm for SBR, and ranged from -0.005 to 0.045 mm on the z-coordinates for ABR and from−0.567 to 0.074 mm for SBR. However, there was no significance in the mean difference between the first and second registrations between the ABR and SBR.
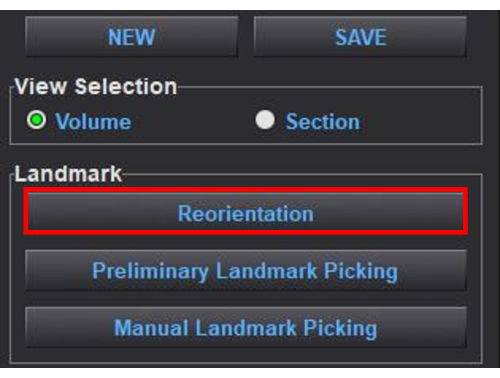
Figure 1: Reorienting a craniofacial model. This is initiated by clicking on the Reorientation button in the Landmark panel. Please click here to view a larger version of this figure.
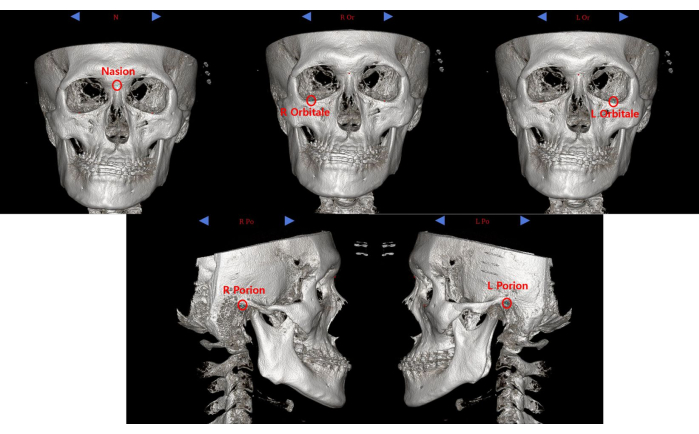
Figure 2: The five basic landmarks for reorientation of the reconstructed craniofacial model; nasion, right and left orbitales, and right and left porions. Please click here to view a larger version of this figure.
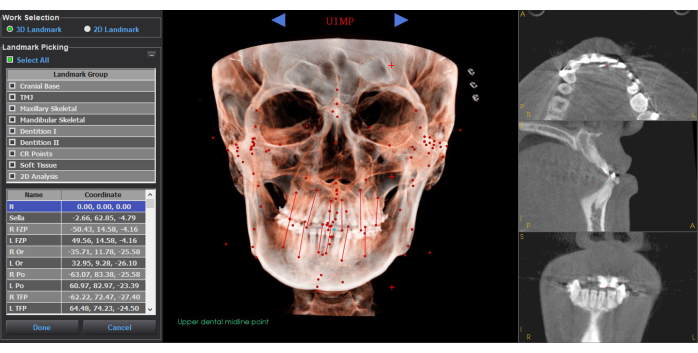
Figure 3: Landmarks and their coordinates after preliminary automatic landmark selection. Reviews and modifications of the landmarks can be done by clicking on the Manual Landmark Picking button in the Volume tab. Please click here to view a larger version of this figure.
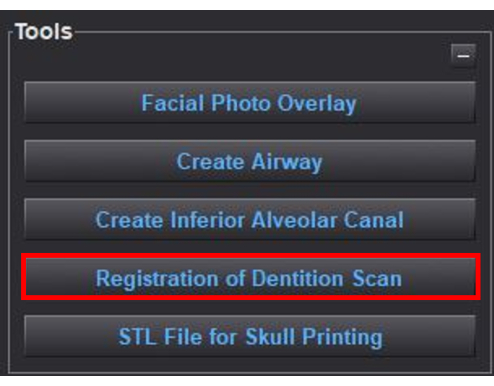
Figure 4: Initiation of merging digital dental images with the reoriented craniofacial model. This is done by clicking on the Registration of Dentition Scan button in the Tools panel. Please click here to view a larger version of this figure.
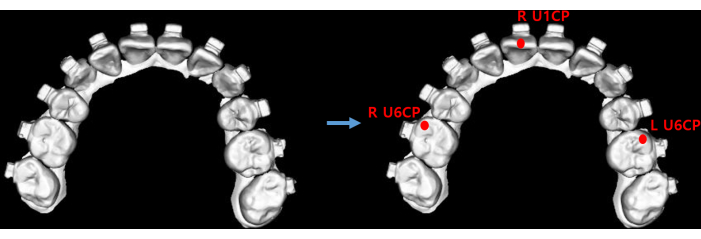
Figure 5: Location of the three registration landmarks on the loaded digital dental images. The mesiobuccal cusps of the right maxillary first molar (R U6CP), the right maxillary central incisor midpoint on incisal edge (R U1CP), and the mesiobuccal cusp of the left maxillary first molar (L U6CP). These landmarks were simultaneously calibrated by machine-learned automation. Please click here to view a larger version of this figure.
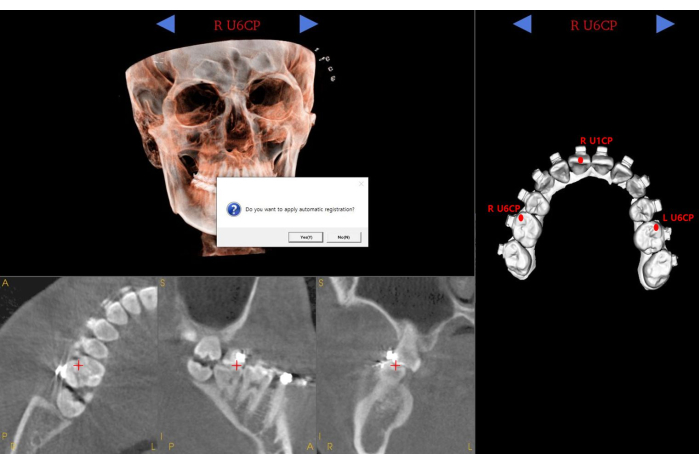
Figure 6: Confirmation of the three registration landmarks on the loaded digital dental images and CBCT. The right and left mesiobuccal cusps of the maxillary first molars (R U6CP, L U6CP) and right upper central incisor midpoint (R U1CP). Clicking on the Yes button performs the automatic registration. Abbreviation: CBCT = cone-beam computed tomography. Please click here to view a larger version of this figure.
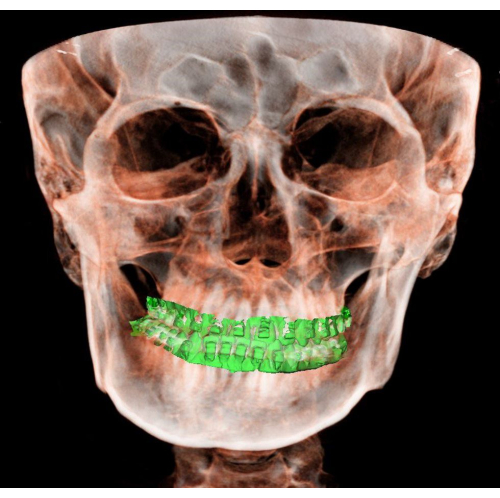
Figure 7: The reconstructed craniofacial model with the digital dental image merged. Please click here to view a larger version of this figure.
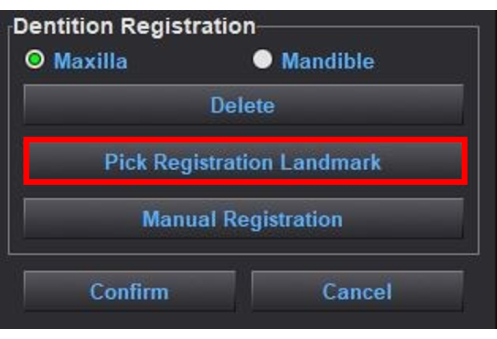
Figure 8: Modifying the merging. When modifying the merging, click on the Pick Registration Landmark button in the Dentition Registration panel. Please click here to view a larger version of this figure.
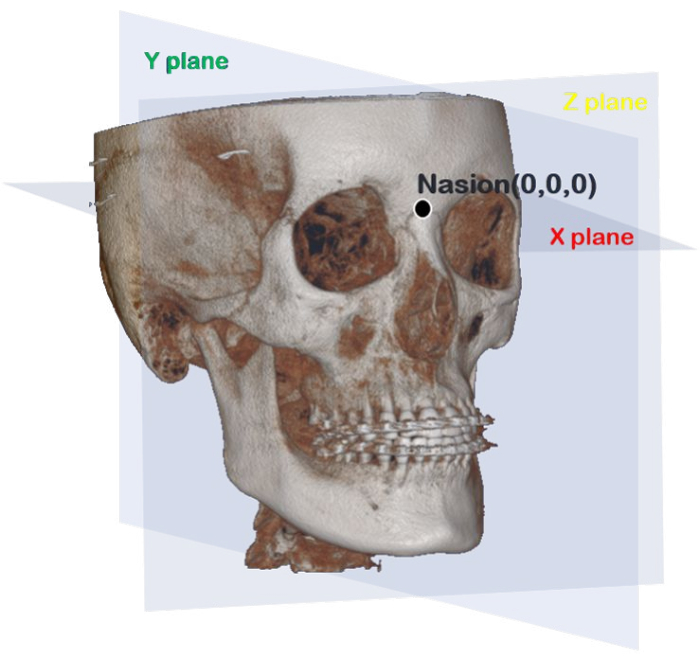
Figure 9: Reference planes of the program. The X-plane (horizontal) is the plane that passes through the Nasion, parallel to the Frankfort horizontal (FH) plane that passes through the left and right Orbitales and right Porion. The Y-plane (midsagittal) is perpendicular to the X-plane, passing through the Nasion and basion. The Z-plane (coronal) sets the plane perpendicular to the horizontal and midsagittal planes via Nasion (zero point; 0, 0, and 0). Please click here to view a larger version of this figure.
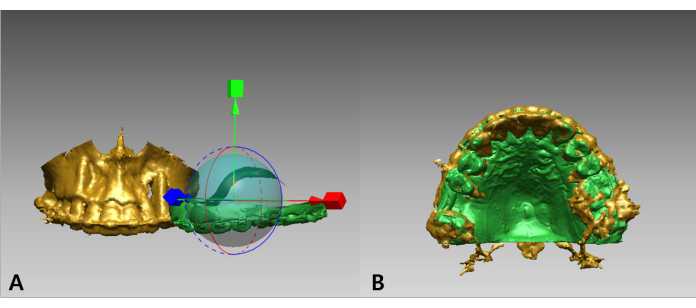
Figure 10: Surface-based registration of the maxillary digital dental images into the dental portions of reconstructed CBCT images. (A) Before and (B) after merging. First, the initial points were registered using the mesiobuccal cusps of the maxillary first molars and the contact point of the central incisors in the CBCT and DDI. Subsequently, the surface was registered to achieve a more accurate integration using the iterative closest points algorithm. Abbreviation: CBCT = cone-beam computed tomography; DDI = digital dental images. Please click here to view a larger version of this figure.
Table 1: Reliability in three coordinates of each landmark when integrating facial CBCTs and digital dental images in each ABR and SBR and between them. *paired t test; †independent t test. ICC > 0.8/0.6/0.4/0.2 or ≤ 0.2 represent very good, good, moderate, fair, or poor strength of agreement, respectively. Abbreviations: CBCT = cone-beam computed tomography; AI = artificial intelligence; ABR = AI-based registration; SBR = surface-based registration; CI = confidence interval; ICC= intraclass coefficient. Please click here to download this Table.
Table 2: The mean differences in the three coordinates of each landmark from repeated registrations of facial CBCTs and digital dental images with the ABR and SBR. Δ (1st-2nd), the mean difference in x, y, and z coordinates of each landmark between the first registration (1st) and second registration (2nd) of DDI and facial CBCT images. *paired t test; †independent t test; bWilcoxon Signed-rank test. Significance was set at P < 0.05. Abbreviations: CBCT = cone-beam computed tomography; AI = artificial intelligence; ABR = AI-based registration; SBR = surface-based registration; S.D. = standard deviation. Please click here to download this Table.
