During the study, one patient received additional other treatments (intra-articular steroid injection) due to increased pain. In one patient, the synovial thickness of the suprapatellar bursae could not be detected on ultrasonography. One patient developed swelling and subcutaneous stasis around the wound after treatment, which improved after ice application without affecting normal treatment and follow-up. Two patients terminated the experiment, and the remaining 58 patients were included in the final statistical analysis.
Baseline features
The participants comprised 27 men and 31 women. Patients ranged in age from 40 to 75 years, with an average age of 57.79 ± 11.33 years. The duration of the disease ranged from 1 to 36 months, with an average duration of 20.78 ± 9.88 months (Table 1).
The synovial thickness of the suprapatellar bursae and VAS and WOMAC scores decreased, and HSS increased after ultrasound-guided acupotomy.
Post-treatment evaluation
After 1 week of treatment, the synovial thickness of the suprapatellar bursae in the treatment group (4.02 ± 0.83) was thinner than that in the control group (5.04 ± 0.67; t =7.978, p < 0.05). After 1 week of treatment, the VAS of the treatment group (4.17 ± 2.07) was significantly lower than that of the control group (6.14 ± 1.80; t = 8.157, p < 0.05). After 1 week of treatment, the WOMAC in the treatment group (38.97 ± 14.28) was significantly lower than that in the control group (59.26 ± 17.32; t = 9.087, p < 0.05). After 1 week of treatment, HSS in the treatment group (73.19 ± 14.75) was significantly higher than that in the control group (56.47 ± 14.47; t = -8.904, p < 0.05; Table 2).
The figures shown here are from the representative case of a 65-year-old female who had recurrent pain in the left knee joint over the past 1 month. Her joint stiffness increased in the morning and was relieved after 10 min of waking. Radiographs of the left knee joint revealed a narrowing of the joint space. The patient met the diagnostic criteria for KOA and voluntarily participated in the study. After contraindications were ruled out, the patient was advised of the possible benefits and risks of ultrasound-guided acupotomy. The patient had a pretreatment VAS score of 7, a WOMAC score of 53, an HSS score of 56, and the synovial thickness of the suprapatellar bursae was 6.5 mm (Table 3 and Figure 3). After 1 week of ultrasound-guided acupotomy, the patient's VAS score was 3, WOMAC score was 40, HSS score was 76, and synovial thickness of the suprapatellar bursa was 3 mm (Table 3 and Figure 4), indicating that the patient's pain, knee function, and synovial thickness of the suprapatellar bursa improved after ultrasound-guided acupotomy.

Figure 1: Prepare materials. All the materials and equipment needed for this operation, including sterilize disposable medical plastic cups, forceps, absorbent cotton balls, self-adhesive dressing, ultrasonic instruments (portable color ultrasound system), sterile ultrasound coupler, sterile protective cover for probe, 40 mm small disposable sterile needle knife, marker pen, disposable medical mask, hygiene hat, type II skin disinfectant, disposable sterile towel, 2% lidocaine hydrochloride, sterile water for injection, 10 mL disposable sterile syringe, sterile needle for injection, and surgical rubber gloves. Please click here to view a larger version of this figure.
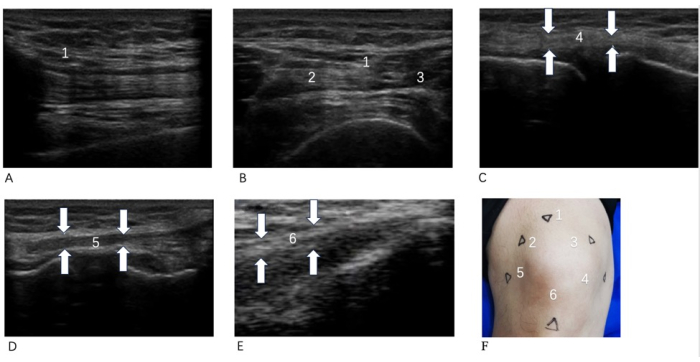
Figure 2: Therapeutic location map. (A) Quadriceps tendon long axis; (B) Quadriceps tendon short axis; (C) Knee tibial collateral ligament long axis; (D) Knee fibular collateral ligament long axis; (E) Patellar tendon long axis; (F) Body surface positioning. 1 Quadriceps tendon stop; 2 Quadriceps medial dilator; 3 Knee tibial collateral ligament; 4 Patellar tendons; 5 Fibular collateral ligaments of knee; 6 Quadriceps lateral dilator. The surface positioning points and ultrasound images of each positioning point for this operation. In (F), 1, 2, and 3 anchor points are in the quadriceps femoris; the long axis of the quadriceps femoris is shown in (A), and the short axis of the quadriceps femoris is shown in (B). Anchor point 4 was in the patellar tendon, corresponding to (C). Fixation point 5 was located in the collateral fibular ligament on the knee side, corresponding to (D). Point 6 is in the tibial collateral ligament on the knee side, corresponding to (E) Please click here to view a larger version of this figure.
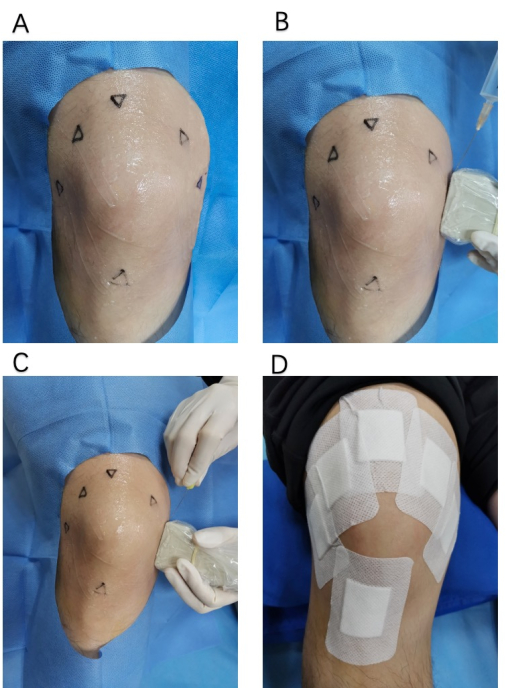
Figure 3: Acupotomy operation diagram. (A) The field of view and the scope of disinfection of the operation ; (B) Local anesthesia under ultrasound; (C) Acupotomy under ultrasound; (D) Postoperative care behavior of protecting the operated wound. Please click here to view a larger version of this figure.
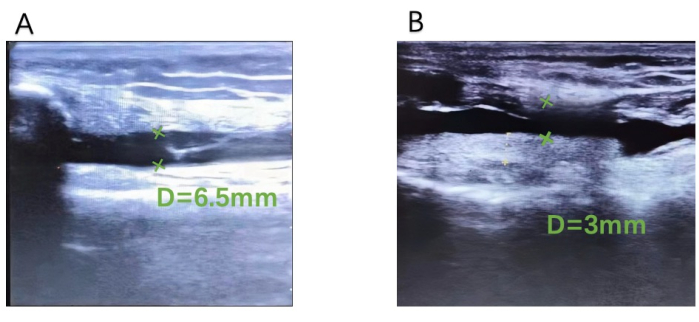
Figure 4: Suprapatellar bursae synovial thickness. (A) Before treatment and (B) after treatment. An ultrasound image of the suprapatellar bursa synovium thickness decreasing from 6.5 mm (A) to 3 mm (B) in the same patient before and after treatment. Please click here to view a larger version of this figure.
Table 1: Baseline information. The basic data of the 58 patients, including gender, mean age, and mean duration of disease. Please click here to download this Table.
Table 2: Scores collected between the treatment and control group. VAS, WOMAC, HSS, and Synovial thickness of suprapatellar bursae were compared between the two groups. For significance calculation, a t-test was used, and the data were expressed as the mean ± SEM. Compared with the control group, * p < 0.05. Please click here to download this Table.
Table 3: Representative patient data. The observation data of one representative patient, including basic information, changes in VAS, WOMAC, HSS, and suprapatellar bursa synovial thickness before and after treatment. Please click here to download this Table.
