1. Setup
- A temperature controlled exam room equipped with an infrared camera and a PC for infrared image acquisition and storage as well as a data acquisition card connected to a computer are shown in Fig.1a.
- The room temperature and skin surface temperature are monitored by thermocouples attached to a data acquisition card during the patient study and measurement data are stored on the computer.
2. Image Acquisition
- Since the lesion cannot be detected in the thermal image without the cooling effect, a square adhesive marker is used to localize the pigmented lesion of interest and its surroundings (Fig. 1b).
- We acquire a bright light image of the pigmented lesion and the adhesive window with a digital camera (Canon PowerShot G11) (Fig. 1b).
- A dermatoscope connected to a digital camera (DermLite Foto System) is used to capture the polarized light image.
- We acquire a steady state infrared image with a Merlin midwave (3-5 μm) infrared camera shown in Fig.1a, c.
- We apply a stream of cold air to the area of the patient’s skin containing the lesion as well as a 50 mm diameter surrounding region for the duration of one minute.
- After one minute, we remove this cooling stress to allow the skin to re-warm at room temperature within 3-4 minutes (thermal recovery phase) (Fig. 1c-d).
- During the thermal recovery phase, infrared images of the pigmented lesion are captured every 2 seconds (Fig. 1c-d).
- All IR images (in addition to the white light and polarized light images) taken during the study are saved and stored using the Labview software.
3. Image Processing
- The IR images are analyzed using a dedicated Matlab code in order to obtain accurate transient temperature distributions on the skin surface. For this purpose, we introduce several calibration steps and a multimodal image analysis system.
- We start with applying a landmark detection algorithm to the bright light image for localizing the corners of the adhesive marker. Next, we identified the corresponding points in the reference IR image.
- In order to compensate for involuntary body/limb movement of the patient, we use these points as landmarks in a quadratic motion model for aligning the IR image sequence during the recovery phase.
- We use the random walker, an interactive image segmentation algorithm where the user can spatially guide the segmentation by placing seed points, to create a mask image delineating the lesion.
- Once we determine the shape of the lesion, we identify the corresponding region in each of the registered IR images.
- We select random points inside the lesion and away from the lesion representing the lesion and the healthy tissue, respectively.
- We compare the transient thermal response of healthy skin and the response of the lesion.
- We prepare a table showing all the data: digital, dermoscopy, color-coded IR images of the lesion and surrounding area recorded at ambient conditions and 2 seconds after the cooling excitation, and the transient thermal response of the lesion and the healthy tissue.
4. Representative Results:
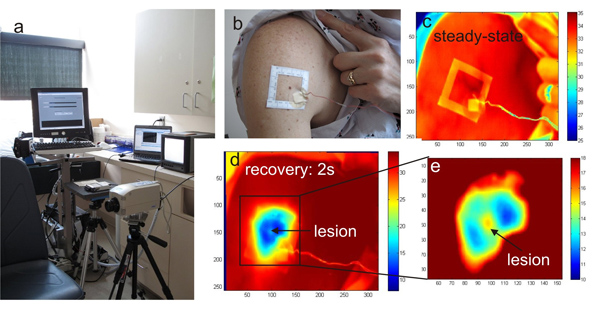
Figure 1. a) The infrared imaging system HRIS in the clinical trial room, b) photograph of the larger body surface area with a cluster of pigmented lesions and the template frame applied for imaging, c) reference infrared image of the region at ambient temperature, d) the same area after cooling and e) magnified section of the melanoma lesion and surroundings
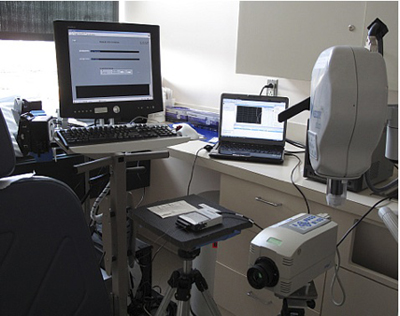
Figure 2. Exam room with our thermal imaging system.

Figure 3. Cooling the lesion and the surrounding skin tissue by blowing a stream of cold air from a vortex tube.
