1. Collection, Storage and Preparation of Serum and Bronchoalveolar Lavage Fluids
- Collect serum from untreated blood samples by allowing blood to clot at 4 °C, and store serum as aliquots at -20 °C prior to use. Bronchoalveolar lavage fluids (BAL) should also be stored as aliquots at -20 °C. Note: Storage of serum and BAL as aliquots limits the potential for degradation of the target antigen by repeated freeze-thawing of samples during repeat testing.
- Thaw samples and mix the serum and BAL samples thoroughly by vortexing and centrifuge for 1 min at 14,000 rpm.
- For routine testing of human serum samples, dilute the serum 1:1 (v/v) with tissue culture medium (TCM). TCM consists of RPMI-1640 medium, 10% (v/v) fetal calf serum, 1% (v/v) of 200mM L-glutamine solution, and sodium azide (0.02% w/v) as preservative. The medium is prepared in advance and can be stored at 4 °C for several months. Apply 100 μl of the diluted serum to the LFD.
- For human BAL fluids, and for BAL fluids from animal models, apply 100 μl of neat sample to the LFD, with no pre-treatment.
- For serum from animal models, dilute serum 1:2 (v/v) with phosphate buffered saline containing 4% (w/v) EDTA, heat for 3min in a boiling water bath, centrifuge for 5 min at 14,000 rpm, and apply 100 μl of neat supernatant to the LFD device.
2. Application of Serum and BAL to the Lateral-flow Device
- Store the lateral-flow devices at room temperature (23 °C). At this temperature, devices are stable for 12 months. Remove the devices from their pouches and place on a level surface.
- Using a sterile pipette tip, apply 100 μl of pre-treated serum or neat BAL sample to the release port of the device.
- Allow the assay to run for 15 min at room temperature, at which time the results of the tests should be recorded. Note: Within seconds the fluid will be seen to migrate by capillary action along the nitrocellulose membrane in the observation window.
3. Recording and Interpreting LFD Results
- The LFD consists of an internal control line (indicated by the letter C on the plastic housing) and a test line (indicated by the letter T). The control line should always appear irrespective of Aspergillus antigen in the serum or BAL sample. This shows that the assay has run correctly.
- If the Aspergillus antigen is present in the serum or BAL sample, the test line will also appear within 15min of sample application. Because the intensity of the test line is proportional to the amount of Aspergillus antigen present in the sample, the test line can appear as a weak positive (+), a moderate positive (++) or as a strong positive (+++). However, any positive test line, regardless of intensity, would indicate the presence of Aspergillus antigen in the sample. In the absence of Aspergillus antigen, no test line will appear, and the result is recorded as negative (-).
4. Representative Results
Representative examples of negative, weak positive, moderate positive, and strong positive LFD results with BAL and serum samples are shown in Figure 1.
Results of antigen-positive LFD tests (weak and strong) or negative LFD tests using BAL fluids from acute myeloid leukemia (AML) patients diagnosed according to EORTC/MSG diagnostic criteria are shown in Table 1. Included in this table are the corresponding clinical and mycological (galactomannan and culture) data, and results of an Aspergillus-specific PCR test developed at St. Bartholomews Hospital8, for each patient. Diagnosis of disease was based on host factors (neutropenia, prolonged use of corticosteroids, treatment with other recognized T-cell immunosuppressants), clinical criteria and GM positivity for BAL (here defined as a GM index value > 0.8). Under the 2002 EORTC/MSG guidelines10, patients 12, 13 and 16 were diagnosed with ‘possible’ IA on the basis of host factors and clinical criteria or GM positivity. According to the revised (2008) EORTC/MSG guidelines2, host factors and GM positivity alone or host factors and clinical criteria alone would not indicate ‘possible’ invasive fungal infection unless accompanied by supporting evidence from clinical data and mycology respectively. Patient 6 was diagnosed with ‘probable’ IA under both 2002 and 2008 guidelines because of host factors, major and minor clinical features and GM positivity. Note, that while neither the LFD nor PCR assays are currently included in EORTC/MSG guidelines, there is strong agreement between the two assays and the commercial galactomannan test indicating the presence of Aspergillus antigen and nucleic acid in the BAL samples of patients 6 and 12. Additional results of trials demonstrating the efficacy of the LFD and PCR assays in diagnosing IPA can be found in Johnson et al8.
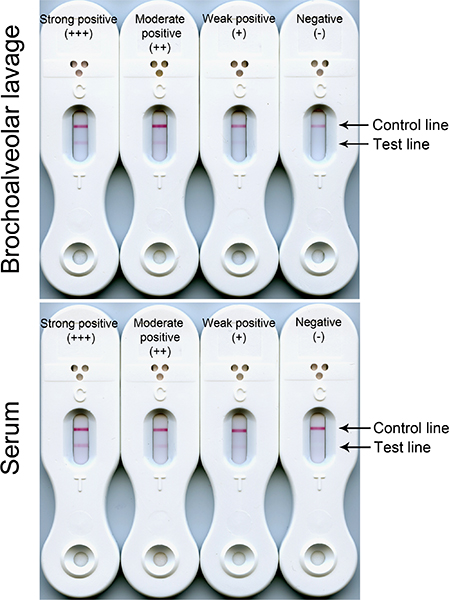
Figure 1. Negative (control line only) and positive (control and test line) results of LFD tests using serum and BAL. The intensities of the test line reactions are proportional to the concentrations of the target antigen in the serum and BAL samples. Reactions typically range from weak (+) through moderate (++) to strong (+++). Regardless of test line intensity, all three serum positive reactions would indicate invasive pulmonary aspergillosis disease due to the presence of circulating Aspergillus antigen in the bloodstream. Positive BAL reactions (weak, moderate or strong) would indicate germination of spores and development of potentially pathogenic hyphae in the lungs.
| Patient no. | Patient information | Clinical criteria1 | BAL culture2 | GM EIA index3 | EORTC / MSG (2002)4 | EORTC / MSG (2008)5 | Aspergillus PCR result | LFD result |
| 6 | – | Major CT signs (nodule and halo) and one minor | Negative | 0.9 (positive) | Probable | Probable | Positive | Weak positive (+) |
| 12 | Presumed previous fungal infection | No major, one minor | Candida glabrata | 6.43 (strong positive) | Possible | None | Positive | Strong positive (+++) |
| 13 | Coagulase-negative Staphylococcus and E. coli in blood | No major, two minor | Negative | 0.25 (negative) | Possible | None | Negative | Negative (-) |
| 16 | Chest infection | 3 minor criteria including new infiltrate plus plural effusion | Negative | 0.16 (negative) | Possible | None | Negative | Negative (-) |
1 Nodules or halos on a computed tomography scan is suggestive of fungal infection
2 Candida glabrata in BAL fluid would be regarded as a contaminant as it is the second most common yeast isolated as part of normal human flora9
3 An index of >0.8 in the GM EIA test of BAL is indicative of Aspergillus infection
4 Based on the 2002 EORTC/MSG diagnostic criteria for ‘possible’, ‘probable’ or ‘proven’ invasive fungal disease10
5 Based on the revised (2008) EORTC/MSG diagnostic criteria for ‘possible’, ‘probable’ or ‘proven’ invasive fungal disease2
Table 1. Results of LFD tests of BAL samples from acute myeloid leukemia patients with probable IPA and from control AML patients (no evidence of infection), and EORTC/MSG diagnosis of infection.
