I. Cell Preparation
- Colorectal cancer cells are grown in culture and harvested when subconfluent.
- A single cell suspension is prepared in phosphate buffered saline and kept on ice.
II. Tumor Preparation
- A mouse with a previously established subcutaneous colorectal tumor is euthanized.
- The subcutaneous tumor is removed using sterile technique and divided into 2-3 mm pieces
- The tumor pieces are kept in phosphate buffered saline on ice.
III. Mouse Preparation
Note: In our laboratory we use inhaled isoflurane to anesthetize the mouse; alternatively, one can use injectable anesthetics to achieve the same effect
- The depth of anesthesia is assessed using toe pinch. There should be no withdraw reflex with toe pinch.
- Antibiotics may be given at this point.
- The anesthetized mouse, which was previously shaved, is properly positioned.
- The abdomen is prepped with a betadine solution.
- The abdomen and surgical site are draped in a sterile fashion.
IV. Laparotomy
- A small nick is made in the skin
- The abdominal wall musculature is grasped and lifted up
- The abdominal cavity is entered and a single blade of the scissors is used to push the intra-abdominal contents away
- The incision is extended to 2-3 cm
V. Exposure of the Cecum
- The cecum with its blind ending pouch is identified and exteriorized
- The cecum is isolated from the rest of the mouse using a pre-cut, sterile gauze
- Warm saline is used to keep the cecum moist
VI. Injection of Cells into the Cecal Wall
- A 27 G or finer needle is used to inject a 50 µL volume of cells into the cecal wall
- The needle is removed
- The injection site is inspected to ensure no leakage
- The cecum is returned to the abdominal cavity
VII. Transplantation of Tumor onto the Cecum
Note: In addition to injecting cells into the cecal wall, an alternative approach is to transplant tumor onto the cecum
- A figure of 8 stitch is placed onto the cecum using 6-0 or 7-0 sized suture
- The cecal wall is lightly damaged
- Then, the tumor piece is positioned
- The stitch is tied down
- The cecum is returned to the abdominal cavity
VIII. Mouse Abdominal Wall Closure and Recovery
- The mouse abdominal wall is closed using three interrupted stitches using 3-0 or 4-0 sized suture
- Alternatively, one can use a simple running stitch
- Post-operative analgesics and a fluid bolus may be given at this point
- The mouse is allowed to recover from anesthesia.
Note: With inhaled anesthetics this typically takes 30 seconds
IX. Results – Primary Tumor and Liver Metastasis

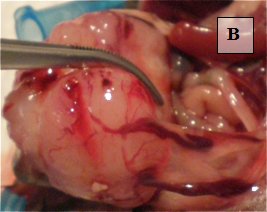
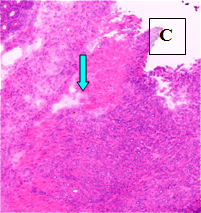
Primary Tumor – shown in situ (A) and with evidence of neovascularization (B); on H&E staining, tumors are locally invasive (C)
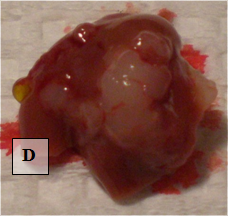
Liver Metastases – shown ex vivo (D)
