The effect of decellularization on whole porcine hearts naturally varies due to differences in size, pressures, and vessel arrangement. Therefore, the exact composition of the derived extracellular matrix scaffolds will not be the same from heart to heart. The completion of the described protocol will yield a heart that appears white or translucent, indicating the loss of cellular material. However, it is widely accepted that a tissue can be considered “decellularized” based on the combination of a few more quantitative parameters 8. A successful decellularization protocol will produce a matrix with less than 50 ng of double stranded DNA per mg of tissue (Figure 6). In order to avoid a host immune response upon implantation of the matrix, the remaining DNA should also contain less than 200 base pairs (Figure 7). To confirm these findings, Hematoxylin and Eosin staining should reveal the absence of nuclear staining in representative sections of the ventricles and ventricular septum (Figure 8). Masson’s Trichrome further confirms the loss of cardiac muscle bundles and retention of collagen networks (Figure 9).

Figure 1. The barbed end of the tubing is inserted into the aorta of the native heart. The tubing must be secured with hose clamps or zip ties above the aortic valve to ensure perfusion through the coronary arteries.
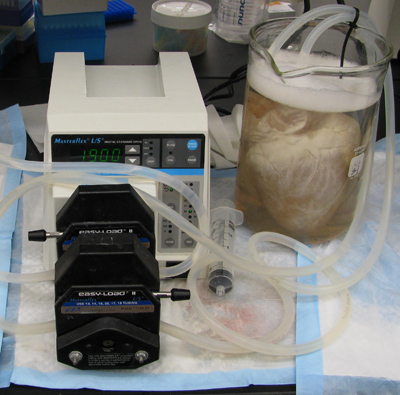
Figure 2. The heart is submerged in water in a 4L beaker and air bubbles must be removed from the tubing. If bubbles are observed emerging from the aorta near the tubing, additional ties must be used to secure the tubing to the aorta in order to maintain adequate pressure in the tissue.
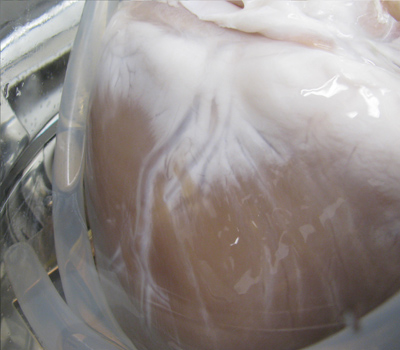
Figure 3. As solutions are perfused through the coronary arteries, the heart will lose its native color, progressing from the atria to the apex of the heart and localized around the coronaries.

Figure 4. After completion of the disinfection and rinse steps of the protocol, the tubing is removed and the heart is placed on an absorbent pad to allow the excess water to drain out of the heart. This ensures an accurate measurement when weighing the tissue and also allows the tissue to relax before sectioning.

Figure 5. The left ventricle (LV), right ventricle (RV), and ventricular septum are all removed from the decellularized heart for histologic processing, freezing and lyophilization, and DNA quantification.
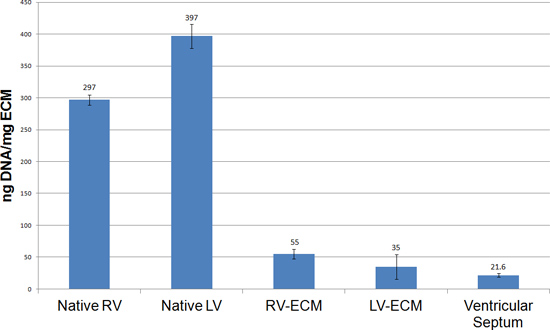
Figure 6. Quantitative analysis of DNA content using a Pico Green assay. The ventricles from cECM hearts show a significant decrease in DNA content when compared to native ventricles. The DNA values observed from this protocol are observed at or below the 50 ng/mg standard for decellularized tissues.
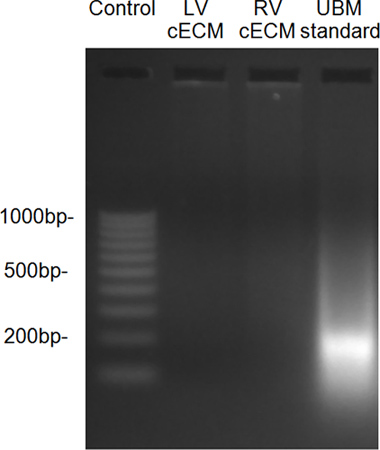
Figure 7. DNA fragment size, as determined by ethidium bromide gel, showed little residual DNA in the decellularized ventricles when compared to a urinary bladder matrix (UBM) standard.
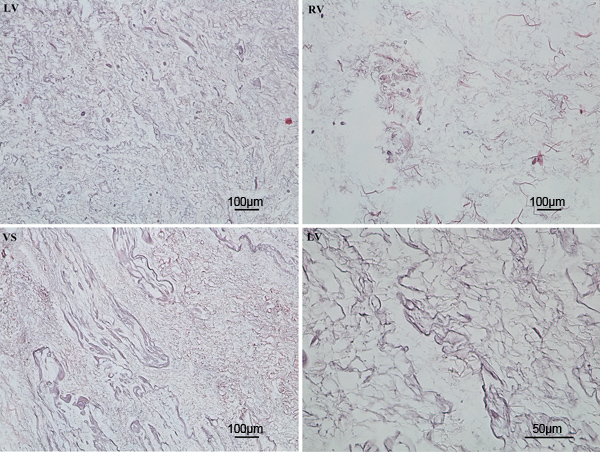
Figure 8. Hematoxylin and Eosin staining showed complete removal of nuclear material from the ventricles following completion of the decellularization protocol.
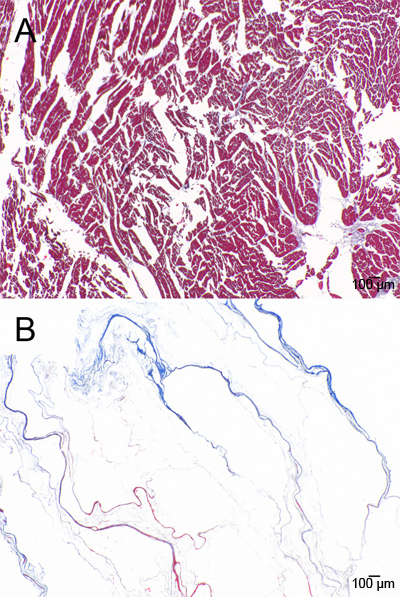
Figure 9. Masson’s Trichrome staining of A) native and B) decellularized ventricle.
