Interpreting and analyzing CED infusions involve several important factors such as distribution fraction and infusate reflux. The distribution fraction calculation depends heavily upon the calculation of the Vd. Therefore accurate interpretation of the MR images is critical. We propose a semi-automated method for reliably reproducing these measurements as listed above. These methods objectively determine the cross sectional area of the infusate cloud and an approximate radius. While variable, in agarose gel the infusion cloud often proved spherical. Assuming a spherical infusate cloud, this radius can be used to determine the Vd for the CED infusion. Vd/Vi for the agarose gel infusion can then be calculated with the measured volume infused. Agarose gel at 0.2% concentration has proven a reasonable representation of brain tissue with a Vd/Vi ratio of 5.0 10, falling in between measured Vd/Vi ratios of brain tissue ranging from 3.1 to 5.2 21,22.
The pressure measurements taken during the CED infusion are also important for ensuring the infusion remains stable and constant. Detected pressure spikes may indicate errors in the infusion such as air bubbles or blockages in the catheter. The pressure profile of the infusion is expected to initially peak before decreasing to a relatively stable plateau for the duration of the infusion20.
The main detriment to the success of the infusion is air in the infusion line. Air alters the measurement of the infusion pressure as well as the volume of the dye being infused. It may also cause local tissue disruption and affect the distribution of the infusate. A successful study was performed using coaxial catheters that yielded parameters to minimize or eliminate the effects produced by air escape into the infusion site23. From our study, we identify a need for future investigations into proper methods of CED infusions using single cannula catheters such as the SmartFlow catheter to equally minimize or eliminate the presence of air.
A key parameter for identifying the presence of air in the infusion line is infusion pressure. As shown by the infusion pressure (mmHg) line in Figure 2, there is a spike in the infusion line pressure at the same time that air is introduced into the catheter line. Comparing the pressure readings to the MR image timestamps, a pressure spike may indicate the presence of an air bubble prior to MR image confirmation. This suggests pressure may be a potential warning marker for detecting and preventing the inappropriate delivery of air in vivo. There was time between the initial spike in pressure and when the air was actually delivered into the gel. That is important to note since air should not be infused into the brain during an actual procedure. If increased pressure was observed in an actual case there might be ample time to keep air from reaching the infusion site within the brain.
Once the air reaches the catheter tip, growth of the air bubble can be seen in the MR images as shown in Figure 3, panels A-F. The air bubble causes enlargement and irregularity of the dye acorn and also alters the measurement of Vd. Thus, it is important to identify and validate a method to prepare the system that consistently ensures it is devoid of air prior to placing the catheter, making certain air does not impair the infusion. One way to prevent air entering the catheter may be to begin the infusion prior to insertion of the catheter into the agarose gel.
Backflow of the infusate along the catheter-gel interface can adversely affect the infusion by allowing the infusate to exit the target. While backflow can occur at any point during an infusion, there is an increased incidence of backflow at the start of the infusion and when increasing the infusion rate10. Backflow has also been associated with the presence of air bubbles, catheter insertion technique, and catheter design, though back flow may still occur despite controlling for these variables23. To minimize backflow, a stepped, reflux resistant catheter was used, and the infusion rate was held constant and as low as possible (1.667 μl/min). One can also avoid unnecessary backflow by preventing pressure spikes. Along with catheter diameter, initial infusion pressure spikes (IIPS) (associated with the expulsion of an end-catheter occlusion) have been shown to increase the probability that backflow will occur. Therefore, a “trickle” technique was used where the infusion was initiated at the minimum rate just prior to insertion. Porous membrane catheters, as well as valve tip catheter designs, have been proposed to mitigate end port occlusions and associated IIPS.
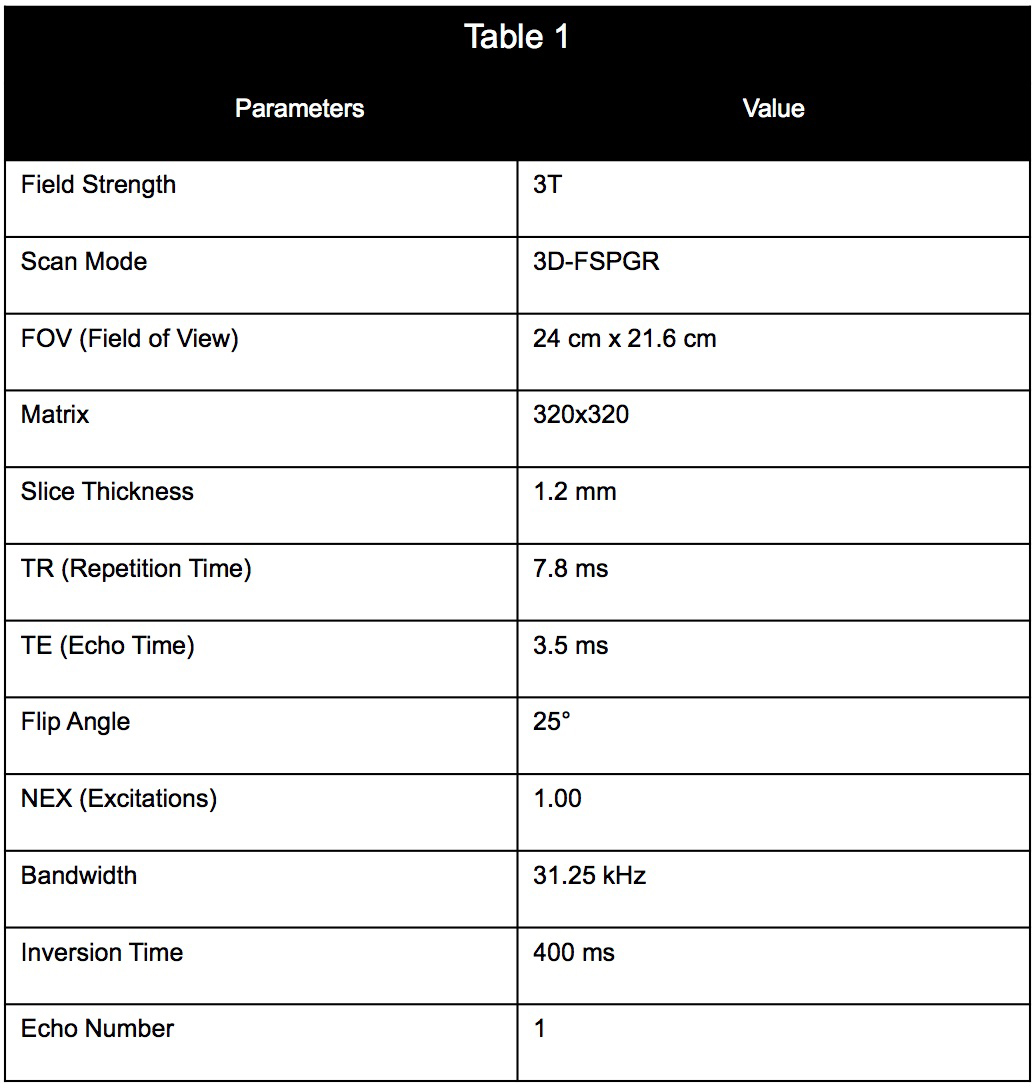
Table 1. Imaging parameters and values used for the MR scan of the infusion.
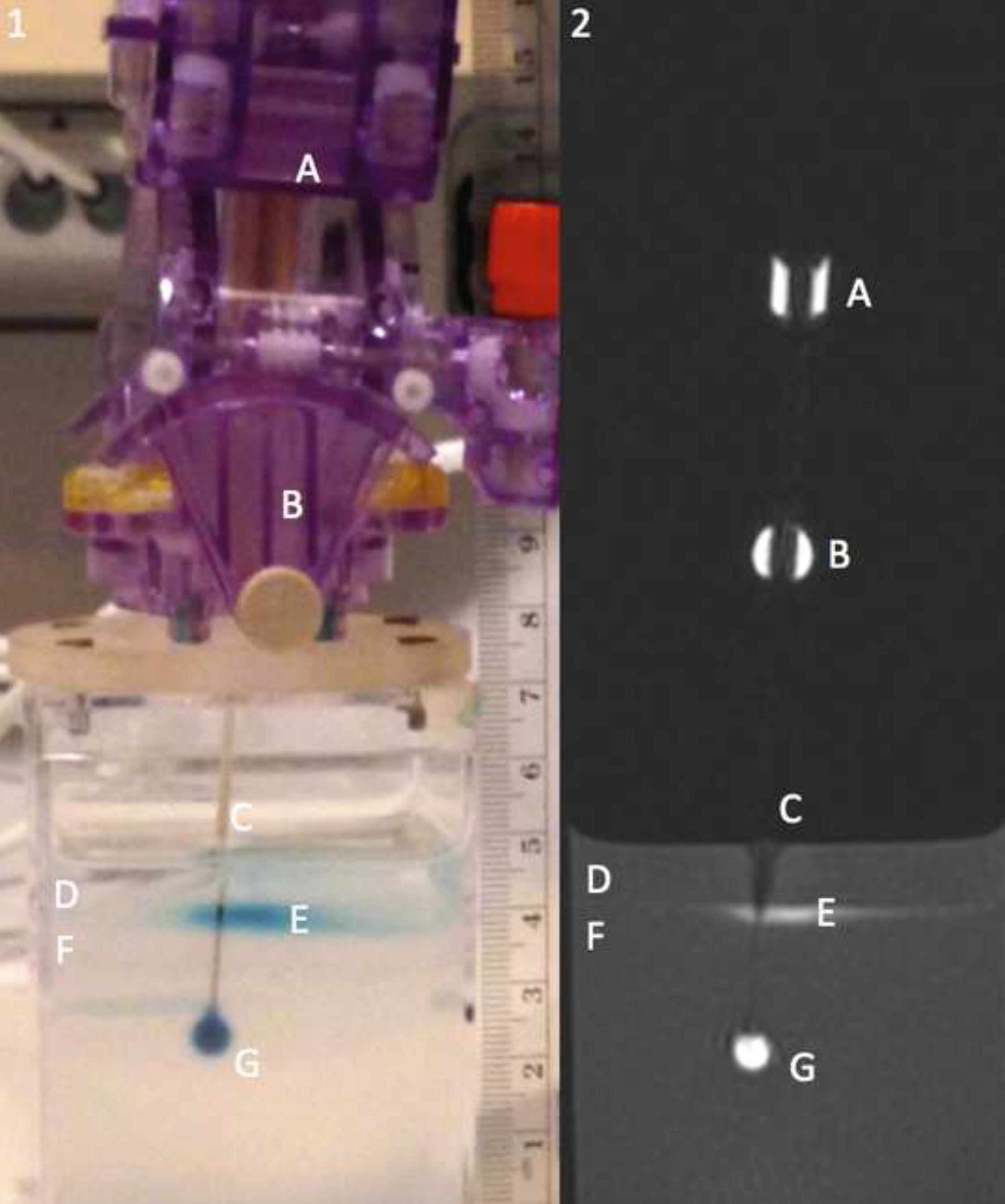
Figure 1. Panel 1 showing a picture of the catheter mount and agarose gel alongside panel 2 containing a MR image of the agarose gel showing a cross section of infusion catheter. Labels as follows: the MR visible trajectory guide can be seen by labels A and B, the infusion catheter by label C, the water on top of the agarose gel by label D, pooling contrast agent at the gel water interface by label E, the agarose gel by label F, and the infusion cloud by label G.

Figure 2. Graph demonstrating the effects of air on the CED infusion. Air was noted in the infusion line 15 min into the infusion. At 17 min a spike in the pressure was recorded, as shown by the green line. The air bubble also has a drastic effect on the Vd and Vd/Vi ratio as seen by the blue and brown dashed lines respectively. Upon air entering the line, the Vd spiked from approximately 5 to 9 μl; while the Vi remained linear. Please click here to view a larger version of this figure.
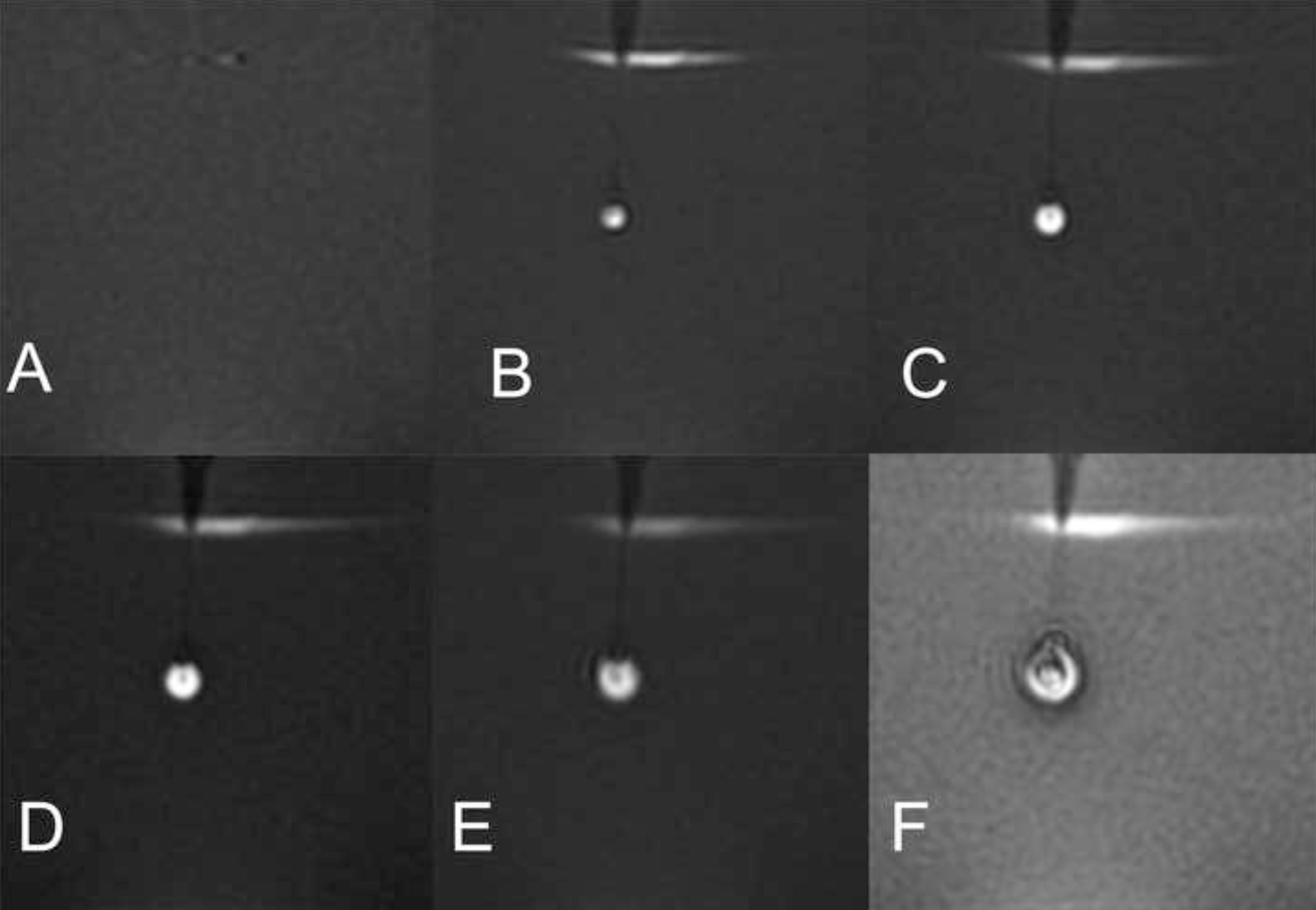
Figure 3. Magnetic resonance images showing growth of the infusion cloud and enclosed air bubble. The first image shows the gel prior to insertion of the catheter, the second image shows the insertion of the catheter after beginning the infusion, and the subsequent time lapse shown is in approximately 4-min intervals. The air bubble distorts the true volume of the infusate cloud and prevents accurate measurement of Vd. Air was seen entering the infusion catheter immediately prior to the MR scan. Panels A-F correspond to points A-F in Figure 2, demonstrating the progression of the infusion.
