The total number of transplanted cells is 1 x 106 cells and was divided into three consecutive injections in the tail vein. We administered 3.3 x 105 cells in 50 µl of phosphate buffer solution (PBS). The first injection was performed within 30 min after injury, the second 6 hr later and the last 18 hr after the lesion. The choice of a time limit of 18 hr after SCI for administering PM-NPCs was determined by the optimal permeability of the blood brain barrier at this time 14. To evaluate the effect of stem cells injection it would be useful to have positive control laminectomies animals (n = 14) and PBS injected animals as a negative control (n = 14).
PM-NPCs Improve Recovery of Hind Limb Function, migrate to lesion site and differentiate in MAP-2 positive cells
The T9 contusion caused the transient loss of hind limb function followed by a progressive gradual recovery (Figure 1). Within 2-3 weeks, PBS-treated injured mice improved and hind limb function reached 3 points of BMS (corresponding to plantar placing of the paw with or without weight support or occasional, frequent, or consistent dorsal stepping, but not plantar stepping 18). Instead, within the same observational period, injured mice treated with PM-NPCs showed a higher recovery, reaching 4.5 points of BMS (corresponding to frequent or consistent plantar stepping without coordination, or frequent or consistent plantar stepping with some coordination). The behavioral improvement was particularly evident in the period between day 7 and day 14 after SCI. No signs of allodynia-like forelimb hyper sensibility 19 were recorded at any time in any experimental group throughout the observational period of 30 days.
Most engrafted PM-NPCs, labeled with PKH26 (Figure 2), accumulated at the edges of the lesion forming clusters (Figure 3) from the early days of their administration. Then the transplanted cells migrated along the lesion edges and in a more diffused fashion where they differentiated, gradually assuming the asymmetric cellular conformation of neurons. At 30 days after lesion and transplantation, the cell body of PM-NPCS increased in size and in most cells dendritic-like processes were obvious and fully immunostained by the specific antibodies to MAP-2 (Figure 4). The achievement of morphological complexity and the positivity to MAP2 by transplanted PM-NPCs is likely not due to fusion with surviving host spinal cord neurons, which is evident in their clearly differentiated morphology and the absence of two nuclei in any single labeled cell.

Figure 1. PM-NPCs improve functional recovery in injured animals. The open field locomotion was the test employed for the determination of motor function recovery 18. Animals were tested the day before the contusion and scored 9 points in the BMS scale. On the first day post injury in the lesioned animals, the BMS score decreased to zero. The recovery of hind limb function of lesioned mice showed a remarkable and long lasting improvement when animals were treated with PM-NPCs. The analysis was performed in double blind, and each group was composed of 14 animals. Values represent average ± SEM. We determined the statistical differences by means of ANOVA test followed by Tukey’s post-test. ***P <0.001; **P <0.01 vs PBS.
Figure 2. PKH26 labeling of PM-NPCS. After labeling procedure with PKH26, PMNPCS are visualized with the live image microscope EVOS fl and photomicrograph was taken with the same instrument (scale bar = 50 µm). Please click here to view a larger version of this figure.
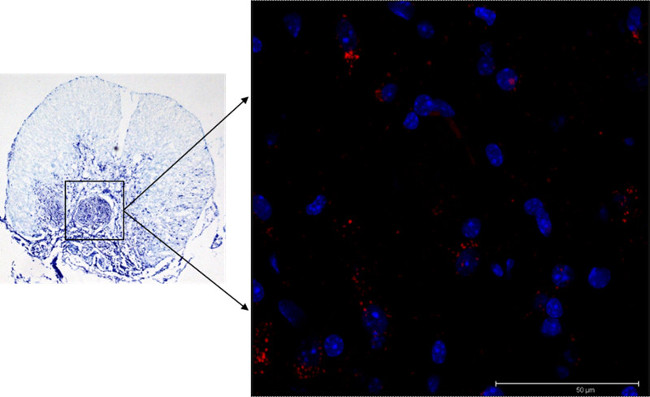
Figure 3. Localization of PM-NPCs in the lesion site. PKH26-labelled PM-NPCs (red) are present throughout the edges of the lesion site at 30 days after their i.v. injection. The image is representative for 1 mouse, but similar images were obtained for at least 5 animals (scale bar = 50 µm). Please click here to view a larger version of this figure.
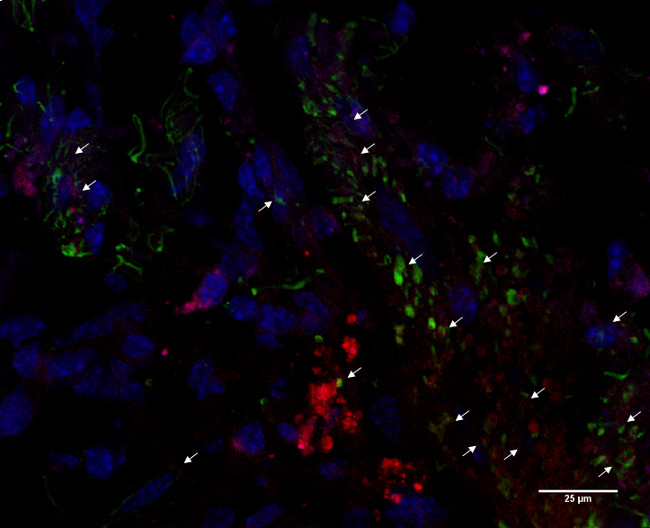
Figure 4. MAP2 expression in transplanted PM-NPCs. Most PKH26-labeled PM-NPCs (red) acquired a neuronal-like shape with dendritic-like processes and had differentiated MAP-2 positive cells (green). Nuclei are stained in blue (DAPI). The image is representative for 1 mouse, but similar images were obtained for at least 5 animals (scale bar = 25 µm). Please click here to view a larger version of this figure.
