This protocol coordinates concurrent acquisition of 3 modalities to capture brain blood flow, electrical muscle activity, and kinematic movement of joints while a participant performs motor tasks (Figure 1).
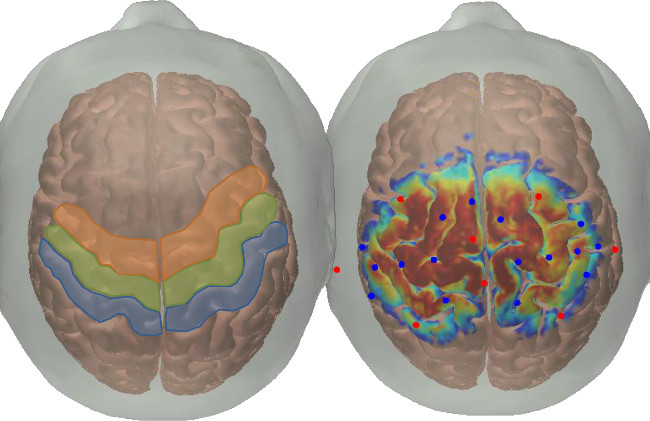
Figure 1. Probe location. The left portion of this figure shows the approximate locations of the sensory areas (in blue, Brodmann areas 1,2,3), the primary motor area (in green, Brodmann area 4), and the premotor area (in orange, Brodmann area 6). The right portion of this figure was generated using AtlasViewerGUI (available for open source download from the MGH Optics Division15) and its associated functions. In brief, this probe design was registered to the surface of the Colin47 Atlas using the spatial arrangement of sources, detectors, and anatomical landmarks (sources are represented by red circles and detectors by blue circles). A Monte Carlo photon migration forward model was run for launching 1 x 108 photons of light through the materials of the skin, skull, and brain, with the sensitivity profiles for all source-detector pairs are projected to the surface of the cortex and all displayed simultaneously in this figure. The color map on the brain’s surface represents the cortical sensitivity of the probe; in other words the number of simulated photons that reach the gyri and sulci located under the sources and detectors (warmer colors indicate more photons than cooler colors, with a range of 2 orders of magnitude on a log 10 scale).
shows an example of source-detector arrangement used in this protocol, and how it is related to underlying neuroanatomical structures on a brain atlas. Figure 2 outlines the block design used in this protocol, as well as screen shots of the instruction videos. Tasks are performed in a block design, with eight 15 sec task blocks interspersed with random length rest periods of 20 – 30 sec. Cartoon animals were specifically chosen to be non human like so as to not engage the mirror neuron system11, and audio cues have been shown to improve task performance in other block design experiments10. The gait task had only an auditory cue, and participants were asked to focus on a small black circle projected onto a screen in front of them.
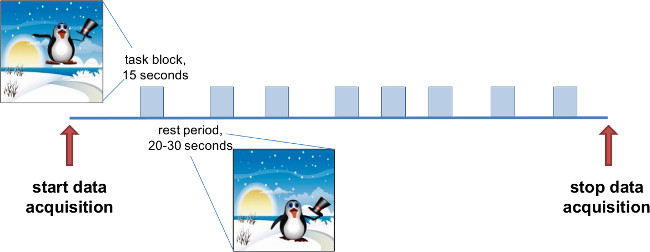
Figure 2. Schematic of each trial. Data collection for each task type lasts approximately 6 min. There are periods of variable rest (ranging between 20 and 30 sec in duration), with 15 sec blocks of activity (gait, cycling, dorsiflexion, or squeezing). Instructional videos were created with visual and auditory cues for the participant to rest or move. The penguin images are taken from one of the instruction videos shown to the patient. He remains on the ground during the rest periods, and jumps in the air 1 time per sec during the task periods. There is also music provided for each condition, a relaxing tune playing during rest and a tune with a strong 60 bpm pace during the task blocks.
Figure 3 is an example of the optical signals recorded during task performance. Data are automatically saved to a file with a *.nirs extension and later transferred from the data acquisition computer for further processing. Figure 4 shows an example of the reconstructed skeletal model, along with joint angle and EMG measures for an ankle dorsiflexion task. The skeletal model and joint angles are created and calculated using Nexus and Visual3D software packages. These data, as well as the EMG have not been processed, and could contain motion artifacts or other noise that could benefit from filtering techniques.
There are a wide array of analysis techniques and software packages available to interpret the data collected. One example is completing fNIRS image reconstruction using an open source software package called HOMer14. An example of the map created is shown in Figure 5 to demonstrate the type of activation information that can be interpreted from the collected optical density signals.
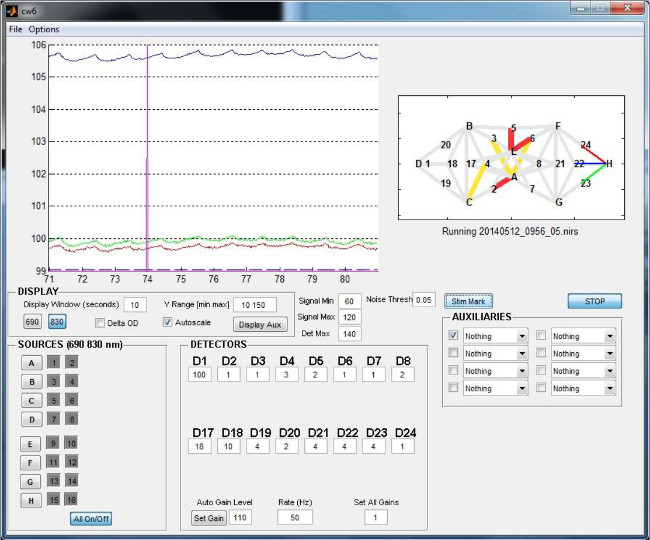
Figure 3. Example of optical density recordings. This screen shot is from the data acquisition software of one type of fNIRS machine. It includes information about the fNIRS probe arrangement (upper right), ability to turn individual laser sources on and off (lower left), and options for modifying the gain of each dectector (bottom middle). In the data visualization window (top left), the vertical pink line represents the start of a block of activity. Colors of the traces correspond to the colors of the channels shown in the probe arrangement on the right. Note that all signals are above 80 dB, and the heart rhythm is clearly visible, even in the light intensity signal.
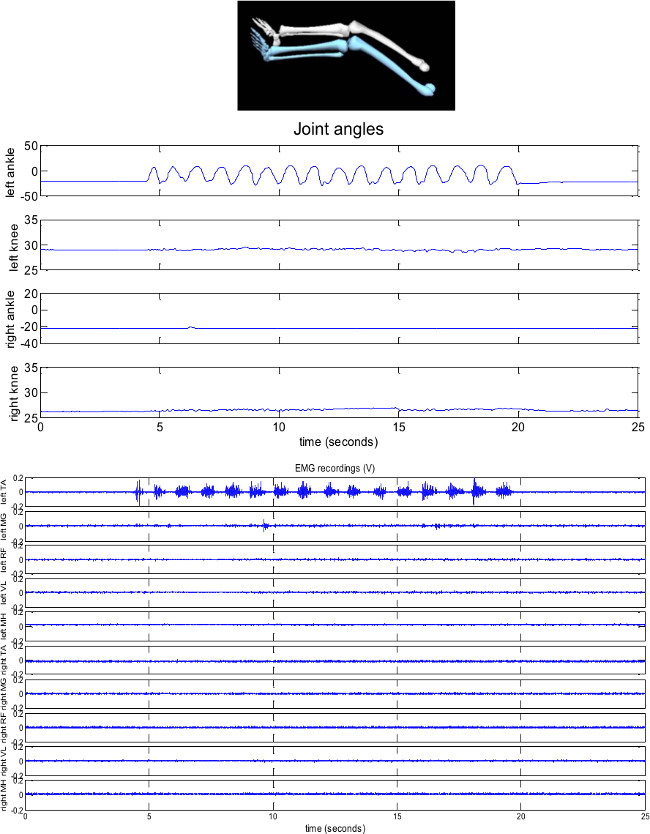
Figure 4. Example skeletal reconstruction, joint angles and EMG for a left dorsiflexion task. The task period during the period represented begins at approximately 4.5 sec, and continues until 19.5 sec. In this typically developing individual (13 years old), there is very limited movement at joints other than the targeted left ankle. In addition, muscles other than the one providing the motion (tibialis anterior) are generally quiescent during the task as well as rest periods. TA = tibialis anterior; MG = medial gastrocnemius; RF = rectus femoris; VL = vastus lateralis; MH = medial hamstrings.
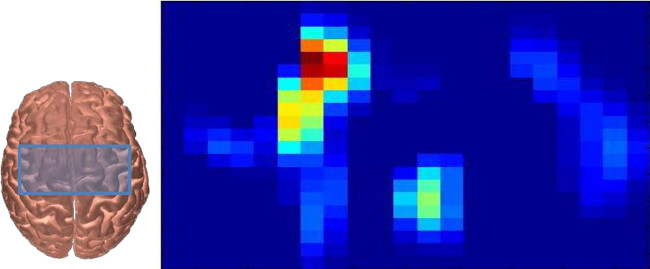
Figure 5. Example of fNIRS activation map during a right handed squeezing task. The blue box on top of the brain outlines the approximate area sampled by this probe design (see also Figure 1). This participant was 13 years old, and had a head circumference of 56 cm). The right portion of the figure shows the average oxygenated hemoglobin (HbO) response during the period 5 – 10 sec following movement onset of one typically developing adolescent squeezing a ball with their right hand. This data in this figure are generated from HOMer14, and then evaluated using a general linear model. The blue colors represent no activation, while the red areas indication regions of increased HbO during the task periods. This is one method of analysis and visualization that researchers use to identify areas of greater changes in oxygenated and/or deoxygenated blood flow.
